Muscle Atrophy: Causes, Symptoms & How to Reverse It
“Your body tears down muscle far faster than it builds it. One week of bed rest — whether from illness or injury — can wipe out the gains from three weeks of consistent strength training.”
This isn’t a worst-case scenario. It’s the biology of muscle atrophy (the medical term for muscle wasting and shrinkage). And it affects millions of people every year, from athletes recovering from injury to older adults experiencing age-related muscle loss.
Left unaddressed, muscle atrophy creates a serious chain reaction: reduced strength leads to functional limitation (difficulty with everyday tasks like climbing stairs or opening jars), which leads to less movement, which accelerates further muscle loss. In older adults, this cycle significantly increases the risk of falls, fractures, and loss of independence.
The good news? In most cases, muscle atrophy is reversible — especially when you act early. In this guide, you’ll learn exactly what muscle atrophy is, what causes it, how to recognize it, and the evidence-based steps you can take to reverse it. We cover 8 key areas: definition and types, causes, symptoms and diagnosis, timeline, treatment and reversal, body-part-specific guidance, neurogenic and pathologic forms, and what to do if your pet is affected.
⚠️ Medical Disclaimer: The information in this article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider (MD, DPT, or specialist) before beginning any exercise or treatment program for muscle atrophy. If you are experiencing sudden, severe, or unexplained muscle weakness, seek medical attention promptly.
Muscle atrophy — the loss of muscle mass and strength — can begin after just 2–3 weeks of inactivity and affects people of all ages (NIH, 2026).
- It starts fast: Significant muscle loss can occur within 2–3 weeks of bed rest or immobilization
- 3 types exist: Disuse (inactivity), Pathologic (disease/aging), Neurogenic (nerve damage)
- The Rebuild Window: Acting within the first 4–6 weeks gives you the fastest, most complete recovery
- It IS reversible: Most cases respond well to progressive resistance training and high-protein nutrition
- See a doctor if: Atrophy is sudden, severe, unexplained, or affects both sides of your body equally
What Is Muscle Atrophy?
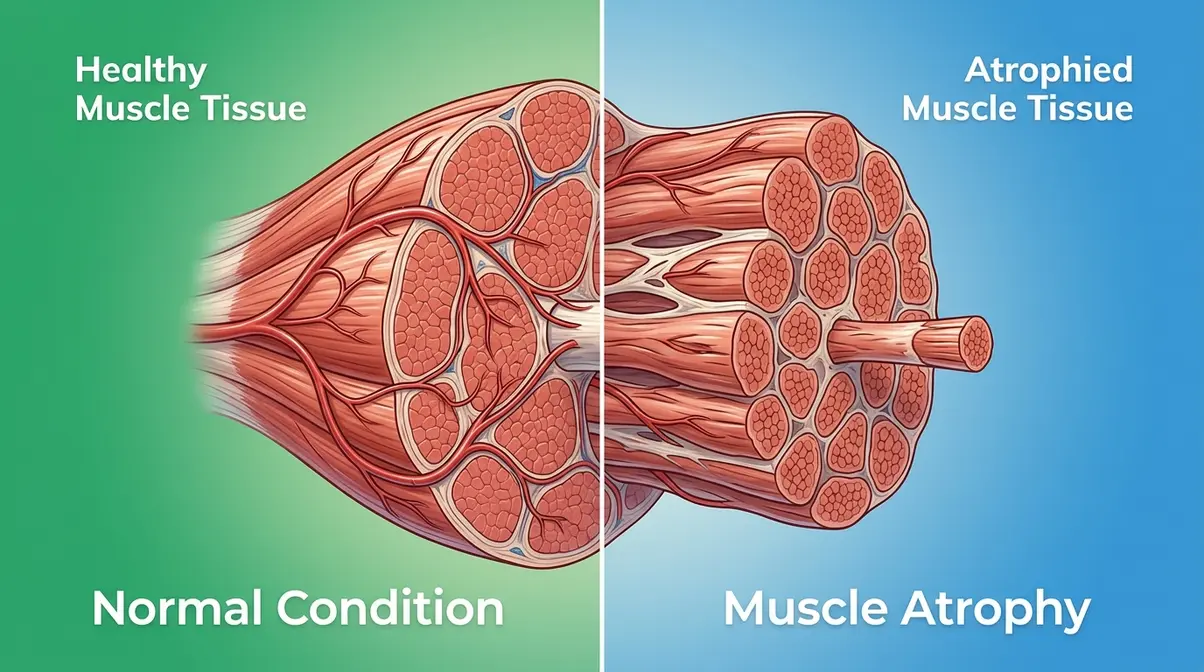
Muscle atrophy is the medical term for the wasting and shrinking of muscle tissue — a process where muscle fibers decrease in size (and sometimes number), causing visible reduction in muscle bulk and a measurable loss of strength. It is not the same as ordinary muscle soreness after exercise. Atrophy reflects a genuine structural change inside the muscle itself.
Think of your muscles like a subscription service. Your body constantly weighs the energy cost of maintaining each muscle against how often that muscle is actually being used. When the muscle isn’t being called upon — due to injury, illness, or simple inactivity — the body “cancels the subscription.” It breaks down muscle protein for fuel or reallocates it elsewhere. This cellular economy is the root of muscle atrophy, and it happens faster than most people realize.
Research from NCBI StatPearls (2026) estimates that muscle atrophy — defined as a measurable decrease in muscle mass due to reduced use, disease, or nerve damage — affects an estimated 30% of adults over 60 worldwide. It is one of the most common complications of hospitalization, prolonged bed rest, and chronic disease.
The Simple Definition of Muscle Atrophy
At its core, muscle atrophy means your muscle fibers are shrinking. Each muscle in your body is made up of thousands of individual fibers. When those fibers are regularly challenged (through movement or resistance), they maintain their size. When they are not challenged, the body reduces their diameter — a process called fiber atrophy — to save energy.
The result is visible: a limb looks thinner, feels weaker, and tires more quickly. According to MedlinePlus, muscle atrophy can result from inactivity, malnutrition, nerve damage, or underlying disease, and it can affect any muscle group in the body.
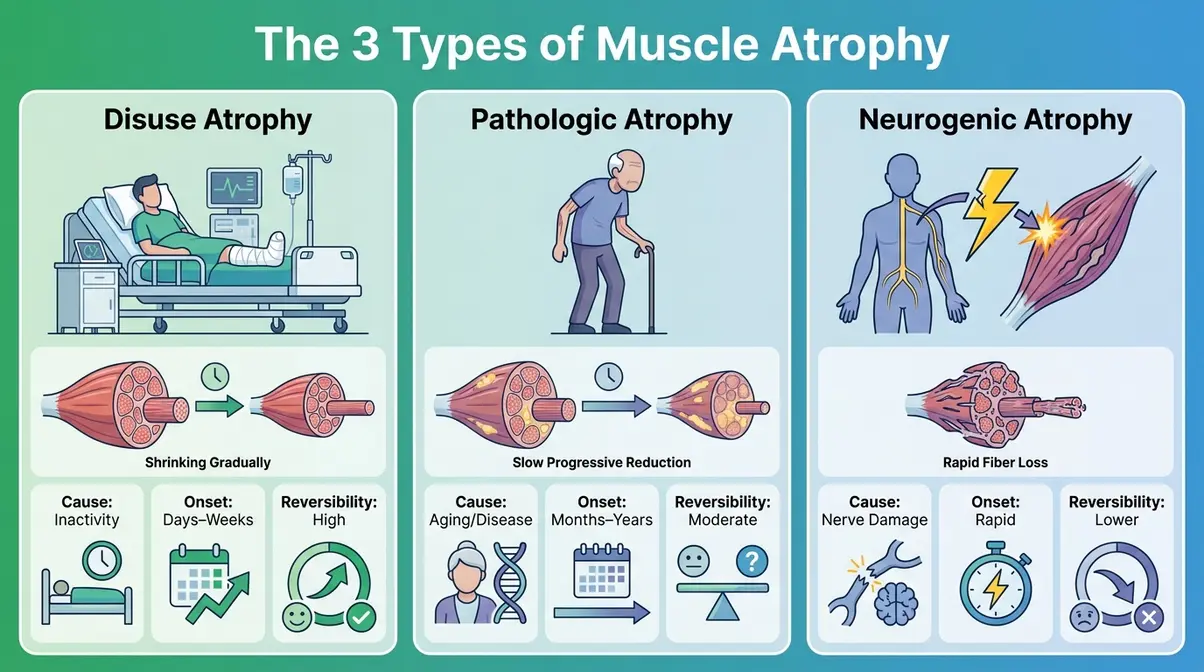
The 3 Types of Muscle Atrophy
Understanding which type you’re dealing with matters — because the treatment approach differs significantly.
| Type | Primary Cause | Common Examples | Reversibility |
|---|---|---|---|
| Disuse Atrophy | Inactivity or immobilization | Bed rest, cast, sedentary lifestyle | High — responds well to exercise |
| Pathologic Atrophy | Disease, aging, or malnutrition | Sarcopenia, cancer, corticosteroid use | Moderate — depends on underlying condition |
| Neurogenic Atrophy | Nerve damage or disease | ALS, spinal cord injury, MS | Lower — requires specialized medical care |
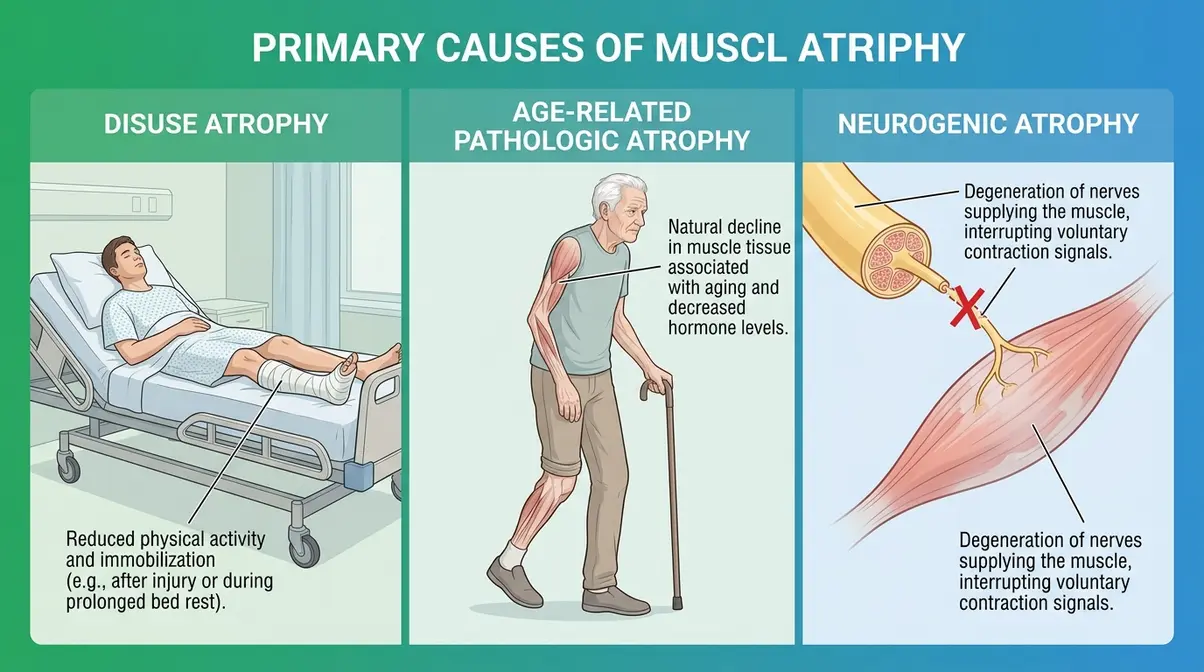
1. Disuse atrophy (muscle loss from inactivity) is the most common form. It occurs when muscles are not used regularly — whether from a broken bone in a cast, weeks of bed rest, or a sedentary lifestyle. This type responds best to rehabilitation.
2. Pathologic atrophy refers to muscle loss caused by a disease process, aging, or nutritional deficiency. Sarcopenia (the age-related form of muscle loss, pronounced sar-koh-PEE-nee-ah) is the most widespread example, affecting an estimated 10–20% of adults over 60 and up to 50% of those over 80 (Journal of Cachexia, Sarcopenia and Muscle, 2026).
3. Neurogenic atrophy (muscle loss caused by nerve damage) is the most serious type. When the nerve supply to a muscle is disrupted — by injury, disease, or conditions like amyotrophic lateral sclerosis (ALS) — the muscle loses its signal to contract and begins to waste rapidly. This form often requires specialized medical intervention beyond standard exercise.
Muscle Wasting vs. Atrophy
These two terms are often used interchangeably, and in most clinical contexts, they mean the same thing. Muscle wasting is the everyday, plain-language term for what medicine calls atrophy. However, some clinicians use “wasting” to describe more severe, systemic muscle loss — the kind seen in advanced cancer, HIV/AIDS, or end-stage kidney disease — whereas “atrophy” can refer to milder, localized loss.
Sarcopenia is a specific subtype: age-related muscle loss that occurs gradually over decades, even in otherwise healthy older adults. It is distinct from atrophy caused by injury or disease, though the end result (smaller, weaker muscles) looks similar.
The bottom line: if you’ve heard the terms “muscle wasting,” “atrophied muscles,” or “shrinking muscles,” they all point to the same underlying process — your body is losing muscle mass faster than it can rebuild it.
What Causes Muscle Atrophy?
Muscle atrophy doesn’t happen randomly. It follows predictable biological pathways, each triggered by a different disruption to the body’s muscle-maintenance system. Physical therapists consistently identify three primary categories of cause: mechanical disuse, systemic disease or aging, and nerve-related disruption. Understanding your specific cause is essential — because the treatment for disuse atrophy is very different from the treatment for neurogenic atrophy.
Disuse Atrophy Explained
Disuse atrophy is the body’s efficiency response to inactivity. When a muscle isn’t being regularly contracted, the body interprets this as a signal that the muscle is no longer necessary at its current size. It begins breaking down muscle protein through a process called proteolysis (protein degradation) — essentially dismantling the muscle fiber from the inside.
This process begins surprisingly quickly. Research published in the Journal of Physiology (2016) found that healthy young adults lost approximately 3.5% of muscle cross-sectional area after just 5 days of complete bed rest. Common triggers include:
- Limb immobilization from fractures, surgery, or casting
- Prolonged bed rest from illness, hospitalization, or surgery recovery
- Sedentary lifestyle — long periods of sitting with minimal physical activity
- Space travel — astronauts lose significant muscle mass in microgravity, making this one of NASA’s primary health challenges
The critical countermeasure is simple in principle: move the muscle. Even partial movement — such as isometric contractions (tensing the muscle without moving the joint) during immobilization — significantly slows disuse atrophy.
Aging, Muscle Loss, and Sarcopenia
Sarcopenia (age-related muscle loss) is an inevitable biological process that begins around age 30 and accelerates after 60. According to the Cleveland Clinic, adults lose approximately 3–5% of muscle mass per decade after age 30, with the rate accelerating significantly after age 60. By age 80, many individuals have lost 30–40% of their peak muscle mass.
Several age-related changes drive this process:
- Declining anabolic hormones — testosterone, estrogen, and growth hormone all decrease with age, reducing the body’s ability to build and maintain muscle
- Reduced satellite cell activity — satellite cells are the muscle’s repair crew; their numbers and responsiveness decrease with age
- Chronic low-grade inflammation — elevated inflammatory markers (like IL-6 and TNF-alpha) in older adults actively promote muscle breakdown
- Reduced appetite and protein intake — many older adults eat less protein, starving the muscle of its primary building material
Sarcopenia is not inevitable in its severity. Clinical evidence from the NIH’s National Institute on Aging indicates that resistance exercise and adequate protein intake can significantly slow or partially reverse age-related muscle loss, even in adults in their 70s and 80s.
Diseases and Medications
Beyond aging and inactivity, a wide range of medical conditions and medications can trigger pathologic atrophy:
- Medical Conditions:
- ALS (amyotrophic lateral sclerosis) — progressive neurogenic atrophy affecting motor neurons
- Multiple sclerosis (MS) — nerve demyelination disrupts muscle signaling
- Muscular dystrophies — genetic conditions causing progressive muscle fiber destruction
- Cancer and cancer cachexia — tumor-related inflammatory signals actively break down muscle
- Chronic kidney disease — metabolic acidosis accelerates protein catabolism
- Diabetes — peripheral neuropathy can trigger neurogenic atrophy in the feet and legs
- Medications:
- Corticosteroids (e.g., prednisone) — one of the most common drug-induced causes of muscle wasting; long-term use suppresses muscle protein synthesis and accelerates breakdown
- Statins (cholesterol-lowering drugs) — can cause myopathy (muscle weakness and pain) in some patients, though severe atrophy is less common
- Certain chemotherapy agents — directly toxic to muscle tissue
If you are taking any of these medications and notice muscle weakness or visible shrinkage, consult your prescribing physician. Never stop a prescribed medication without medical guidance.
Recognizing the Symptoms of Muscle Atrophy
Muscle atrophy rarely announces itself dramatically. More often, it creeps in gradually — a limb that looks thinner, a grip that feels weaker, stairs that feel harder than they used to. Across clinical practice, physical therapists report that many patients don’t recognize atrophy until it has already progressed for weeks or months. Catching it early — ideally in those first few weeks — is what determines how quickly and completely you recover.
First Signs to Watch For
The earliest symptoms of muscle atrophy are often subtle and easy to dismiss as fatigue or normal aging. Research from Medical News Today and MedlinePlus identifies these as the most consistent early warning signs:
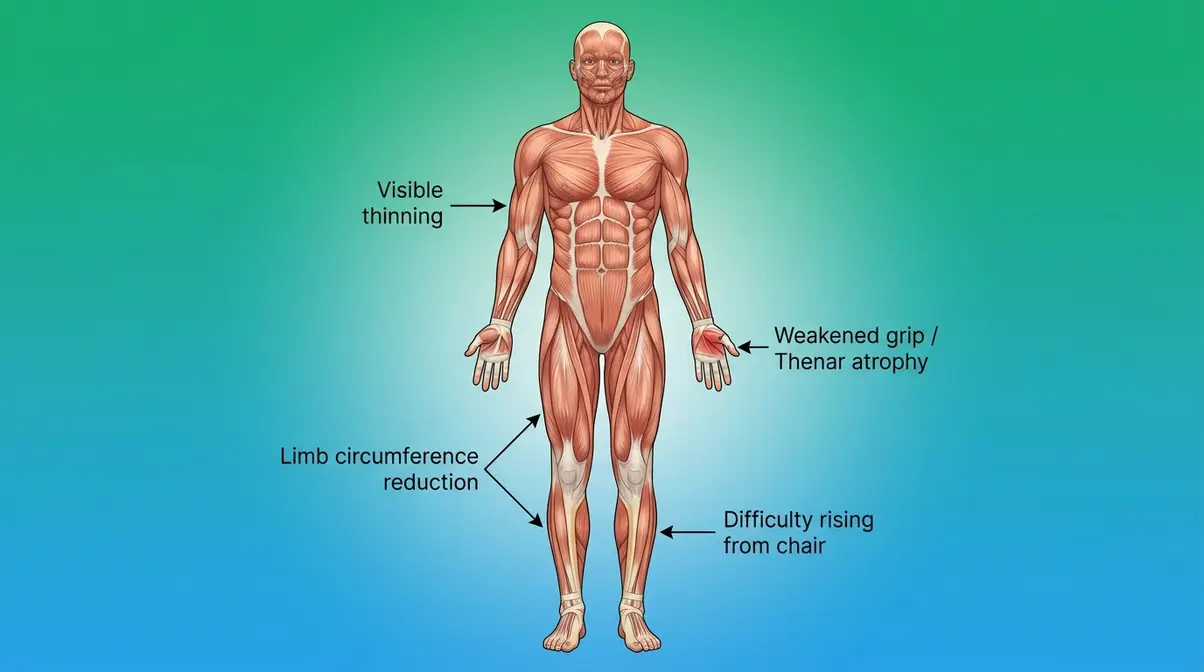
- Visual signs:
- One limb (arm or leg) appears noticeably thinner or smaller than the other
- Visible hollowing or “caving in” around a muscle group (especially the thighs, calves, or upper arms)
- Clothing fits differently — a sleeve or pant leg that was once snug now feels loose
- Functional signs:
- Weakness in a specific muscle group — difficulty lifting objects you previously managed easily
- Increased effort required for everyday tasks: climbing stairs, rising from a chair, opening containers
- Reduced balance or coordination, particularly in the lower body
- Sensory signs:
- A feeling of heaviness or fatigue in the affected limb after minimal exertion
- Muscle cramping or twitching (particularly with neurogenic atrophy)
Why this matters: The earlier you catch these signs, the shorter your recovery window. Atrophy that has been present for 2–3 weeks responds far better to rehabilitation than atrophy that has been building for 6 months.
Pain and Sensory Changes
This is one of the most common questions people ask — and the answer depends on the type of atrophy. Disuse atrophy itself is typically painless. The muscle simply becomes smaller and weaker without generating significant pain signals. You may notice aching or fatigue after minimal exertion, but the atrophy process itself is not acutely painful.
Neurogenic atrophy, however, is often accompanied by pain, burning, tingling, or numbness — because the nerve damage that causes the atrophy also disrupts normal sensory signaling. Conditions like peripheral neuropathy or a herniated disc may cause sharp or shooting pain alongside muscle wasting.
Pathologic atrophy from inflammatory conditions (like polymyositis, an inflammatory muscle disease) can be genuinely painful, with muscle tenderness and soreness even at rest.
The practical rule: if your muscle loss is accompanied by significant pain, burning, or numbness, see a doctor promptly. These symptoms suggest nerve involvement or an underlying inflammatory condition that needs diagnosis before treatment.
How Doctors Confirm Atrophy
If you or your doctor suspect muscle atrophy, a structured diagnostic process typically follows. According to the Cleveland Clinic, standard diagnostic tools include:
- Physical examination — comparing muscle bulk, strength, and reflexes on both sides of the body; measuring limb circumference with a tape measure
- Blood tests — checking for elevated creatine kinase (CK, a marker of muscle damage), inflammatory markers, thyroid function, and nutritional deficiencies
- Electromyography (EMG) — measures the electrical activity of muscles and can identify whether the cause is muscular or neurological
- Nerve conduction studies (NCS) — assess the speed and strength of electrical signals along peripheral nerves
- MRI or ultrasound — imaging can directly visualize muscle bulk, fat infiltration, and structural changes within specific muscle groups
- Muscle biopsy — in cases of suspected inflammatory or genetic muscle disease, a small tissue sample may be analyzed under a microscope
Bring a written record of when you first noticed symptoms, which muscles are affected, any recent injuries or illnesses, and a complete medication list to your appointment. This information significantly speeds up the diagnostic process.
Timeline and Progression
Understanding the timeline of muscle atrophy is one of the most anxiety-reducing things you can learn. Yes, muscle loss begins faster than most people expect. But the body also has a remarkable built-in advantage for rebuilding — if you act within the right window.
How long does it take for muscles to atrophy?
Understanding the timeline of muscle atrophy is one of the most anxiety-reducing things you can learn. If you are wondering how quickly do you lose muscle, the answer depends on your activity level, but measurable muscle atrophy can begin within 3–5 days of complete inactivity. Significant size and strength loss becomes visible by weeks 2–3.
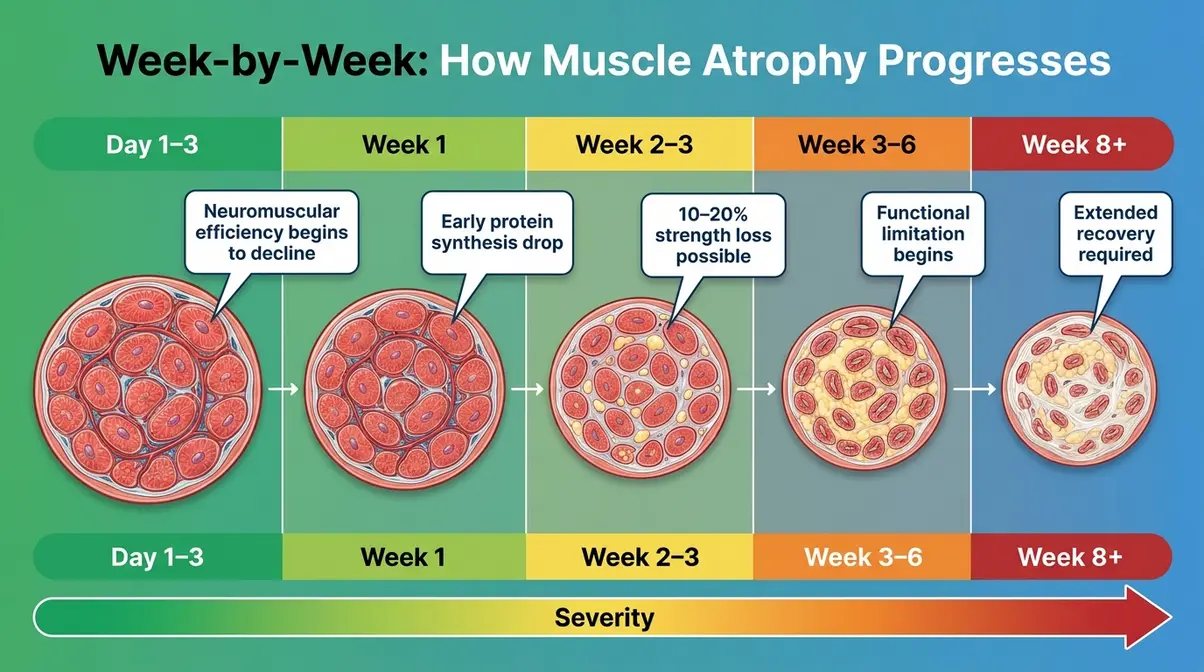
The timeline of disuse atrophy is well-documented in clinical research. Here’s what the evidence shows:
| Timeframe | What Happens | Clinical Evidence |
|---|---|---|
| Days 1–3 | Neuromuscular efficiency begins to decline; strength drops slightly even before visible size loss | Wall & Dirks, J Physiology, 2013 |
| Week 1 | Measurable reduction in muscle protein synthesis; early fiber shrinkage begins | Ferretti et al., Pflügers Archiv, 2001 |
| Weeks 2–3 | Visible reduction in muscle size; strength loss of 10–20% possible in previously immobilized limbs | Kortebein et al., JAMA, 2007 |
| Weeks 3–6 | Continued fiber shrinkage; significant functional limitation; fat begins to infiltrate muscle tissue | English & Paddon-Jones, Curr Opin Clin Nutr, 2010 |
| Beyond 6 weeks | Progressive atrophy; recovery becomes longer and more demanding | NIH, National Institute on Aging |
The most alarming finding from this research: older adults lose muscle 2–3 times faster than younger adults during bed rest. A study by Kortebein et al. published in JAMA (2007) found that adults over 67 lost an average of 1 kg (2.2 lbs) of lean muscle mass after just 10 days of bed rest — a loss that took over 30 days of rehabilitation to partially recover.
The Science of Reversal

Here is the most important message in this entire guide: for most people, muscle atrophy is not permanent.
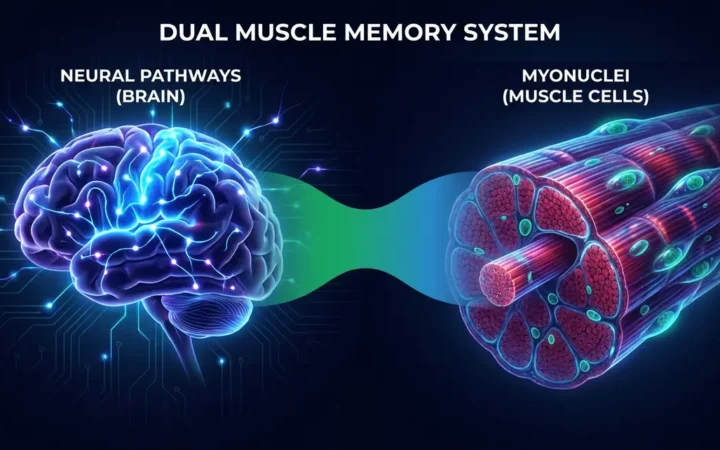
The scientific basis for this optimism lies in a phenomenon called muscle memory — more precisely, the retention of myonuclei (the cellular control centers within muscle fibers) even after atrophy occurs. When a muscle shrinks, it doesn’t lose all of its myonuclei. These nuclei remain dormant, waiting for the signal to rebuild. When training resumes, the muscle can rebuild faster than it could grow from scratch — sometimes 2–3 times faster (Gundersen, Journal of Experimental Biology, 2016).
This is the foundation of “The Rebuild Window” — the critical 4–6 week period immediately following the onset of atrophy during which the body’s residual myonuclei are most active and responsive to rehabilitation. Research suggests that individuals who begin structured resistance training and adequate protein intake within this window achieve significantly faster and more complete recovery than those who wait months before acting.
The Rebuild Window in practice:
- Week 1–2 post-onset: Begin gentle movement; isometric exercises if the limb is immobilized
- Week 2–4: Progress to range-of-motion and light resistance exercises under professional guidance
- Week 4–6: Structured progressive resistance training; protein intake optimized (discussed in H2 #5)
- Beyond 6 weeks: Recovery is still possible, but the timeline extends significantly
The key message: acting early is not just helpful — it is the single most powerful variable in determining how fast and fully you recover.
Treatment and Reversal Protocol
Reversing muscle atrophy requires a three-pronged approach: mechanical stimulus (exercise), nutritional support (protein and calories), and — in severe cases — medical intervention. Physical therapists and clinical researchers consistently report that the combination of resistance training and adequate protein intake produces the fastest and most durable recovery outcomes.
Can you fix atrophied muscles?
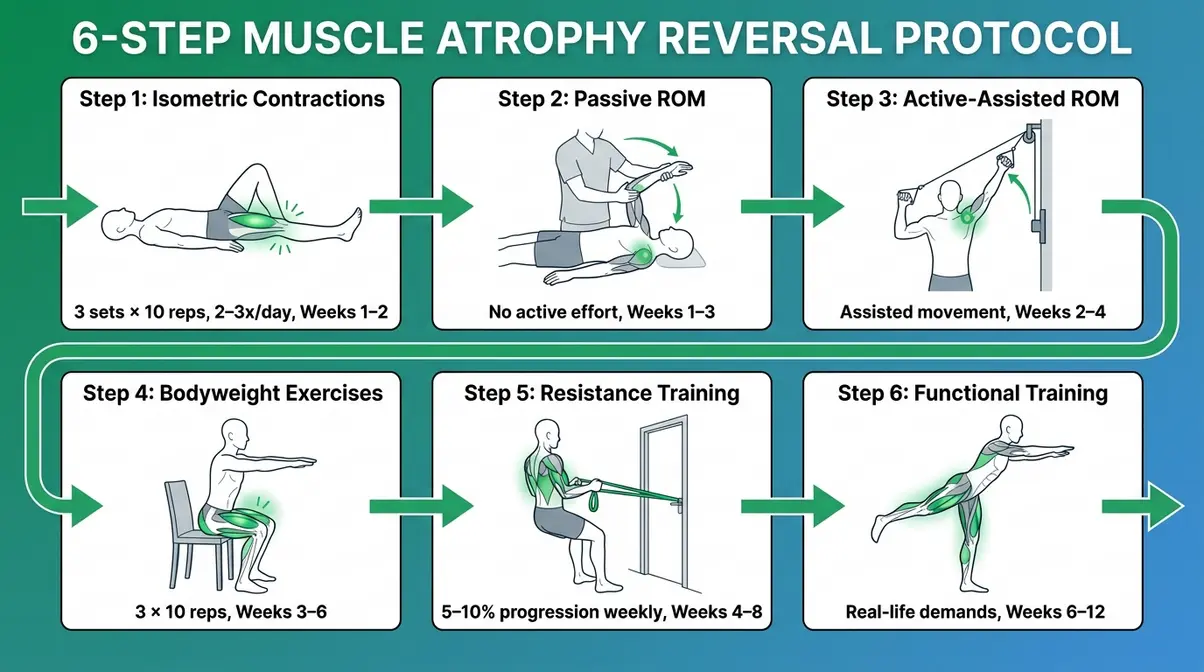
Yes—most cases of muscle atrophy are reversible, and fixing atrophied muscles requires a structured approach. This 6-step protocol is organized by progression — start at Step 1 and advance only when you can complete each step with good form and minimal fatigue. Always consult a licensed physical therapist (DPT) before beginning, particularly if your atrophy is the result of injury, surgery, or neurological disease.
- Step 1: Isometric Contractions (Weeks 1–2)
- Best for: immobilized limbs, immediate post-surgery, severe weakness
- Tense the target muscle without moving the joint (e.g., tighten your quadriceps while keeping your leg straight)
- Hold for 5–10 seconds, release, repeat 10 times
- Perform 3 sets, 2–3 times per day
- Why this matters: Isometric contractions maintain neuromuscular connections and slow fiber atrophy even when the joint cannot move
- Step 2: Passive Range of Motion (Weeks 1–3)
- Best for: patients with very limited strength or post-surgical restrictions
- A therapist or caregiver gently moves the affected limb through its full range of motion
- No active muscle effort required from the patient
- Why this matters: Prevents joint stiffness and maintains tissue extensibility while the muscle begins to recover
- Step 3: Active-Assisted Range of Motion (Weeks 2–4)
- Best for: patients beginning to regain some voluntary control
- Patient actively attempts the movement while a therapist or gravity-assist device helps complete the range
- Example: Using a pulley system to assist a weakened shoulder through overhead motion
- Why this matters: Begins reactivating dormant motor units (groups of muscle fibers controlled by a single nerve)
- Step 4: Bodyweight Resistance Exercises (Weeks 3–6)
- Best for: mild to moderate disuse atrophy with full joint mobility
- Chair squats: Stand in front of a chair, lower slowly until seated, stand back up. 3 sets × 10 reps.
- Wall push-ups: Hands against wall, perform push-up motion. 3 sets × 10 reps.
- Heel raises: Stand behind a chair for balance, rise onto toes. 3 sets × 15 reps.
- Why this matters: Bodyweight exercises provide sufficient mechanical stimulus to trigger muscle protein synthesis without overloading recovering tissue
- Step 5: Progressive Resistance Training (Weeks 4–8+)
- Best for: moderate atrophy with good baseline mobility
- Begin with resistance bands or light dumbbells (1–3 kg / 2–6 lbs)
- Increase resistance by 5–10% every 1–2 weeks as strength improves
- Focus on compound movements: squats, rows, presses, deadlifts (modified as needed)
- Why this matters: Progressive overload is the primary mechanical signal that triggers long-term muscle hypertrophy (growth)
- Step 6: Functional Movement Training (Weeks 6–12+)
- Best for: late-stage recovery; preparing for return to daily activities or sport
- Exercises mimic real-life demands: stair climbing, carrying loads, balance challenges
- Include balance training (single-leg stands, wobble board) to rebuild proprioception (the body’s sense of position)
- Why this matters: Functional strength — not just muscle size — is the ultimate goal of atrophy rehabilitation
Nutrition to Rebuild Muscle
Exercise provides the mechanical stimulus for muscle growth — but without the right nutritional environment, the body cannot rebuild effectively. Research from the American Journal of Clinical Nutrition (2026) and NIH guidelines identify protein intake as the single most critical dietary variable in atrophy recovery.
Protein Recommendations:
| Population | Recommended Daily Protein Intake | Source |
|---|---|---|
| Sedentary healthy adults | 0.8 g/kg body weight | WHO/RDA standard |
| Adults recovering from atrophy | 1.2–1.6 g/kg body weight | ISSN Position Stand, 2017 |
| Older adults (60+) with sarcopenia | 1.6–2.0 g/kg body weight | ESPEN Guidelines, 2026 |
| Post-surgical / severe atrophy | Up to 2.0–2.5 g/kg body weight | Clinical nutrition guidelines |
For a 70 kg (154 lb) adult recovering from atrophy, this means consuming 84–112 grams of protein per day at minimum — roughly double the standard dietary recommendation.
Key nutritional principles for muscle rebuilding:
- Distribute protein across meals. Consuming 30–40 grams of protein per meal maximizes muscle protein synthesis. Spreading intake across 4 meals is more effective than eating the same total in 1–2 large meals (Areta et al., Journal of Physiology, 2013).
- Prioritize leucine-rich protein sources. Leucine is the amino acid most responsible for triggering muscle protein synthesis. High-leucine foods include: whey protein, chicken, beef, eggs, and soybeans.
- Time protein around exercise. Consuming 20–40 grams of protein within 2 hours of resistance training amplifies the muscle-building response (International Society of Sports Nutrition, 2017).
- Ensure adequate total caloric intake. A caloric deficit suppresses muscle protein synthesis even when protein intake is adequate. Unless weight loss is a specific medical goal, recovering from atrophy requires maintenance or slight surplus calories.
- Supplement strategically if needed. Creatine monohydrate (3–5 g/day) has strong evidence (Cochrane Review, 2012) for improving muscle strength and lean mass gains in older adults when combined with resistance training. Vitamin D deficiency is also associated with accelerated muscle loss — get levels tested if you are over 60 or have limited sun exposure.
Medical Treatments for Atrophy
When muscle atrophy is caused by an underlying medical condition — particularly neurogenic atrophy from nerve damage — exercise alone is insufficient. Medical treatment of the root cause is the first priority.
Medical interventions may include:
- Neuromuscular electrical stimulation (NMES): Electrodes placed on the skin deliver mild electrical pulses that artificially stimulate muscle contractions in paralyzed or denervated muscles. Clinical evidence from PMC (Maffiuletti, European Journal of Applied Physiology, 2010) supports NMES for maintaining muscle mass in patients who cannot voluntarily contract muscles.
- Hormone therapy: In cases of severe sarcopenia with documented testosterone deficiency, supervised testosterone replacement therapy may be considered. This is a medical decision — not a self-treatment option.
- Corticosteroid tapering: For drug-induced atrophy from long-term steroid use, a medically supervised taper of the corticosteroid dose (combined with exercise) can partially reverse muscle loss.
- Disease-specific treatments: ALS, MS, and muscular dystrophies each have specialized treatment protocols managed by neurologists and specialist teams. Early referral to a neuromuscular disease center is critical.
How to Prevent Muscle Atrophy
Prevention is significantly easier than reversal. Implementing strategies to prevent muscle loss during a cutting phase or period of inactivity is crucial. The evidence-based critical countermeasures against muscle atrophy include:
- Resistance train at least 2–3 times per week — even low-intensity resistance exercise (elastic bands, bodyweight) is sufficient to maintain muscle mass in sedentary adults
- Meet daily protein targets — 1.2–1.6 g/kg body weight for active adults; 1.6–2.0 g/kg for adults over 60
- Stay active during illness — if bed rest is unavoidable, perform isometric contractions and range-of-motion exercises daily
- Request early mobilization after surgery — ask your surgical team about getting out of bed within 24 hours post-surgery; early ambulation reduces post-surgical atrophy significantly
- Manage chronic conditions — controlling blood sugar, inflammation, and hormonal imbalances reduces the disease-related drivers of pathologic atrophy
Atrophy in Specific Body Parts
While muscle atrophy can affect any muscle group, certain areas are disproportionately common — and each presents with slightly different symptoms and requires targeted rehabilitation strategies.
Leg, Calf, and Thigh Atrophy
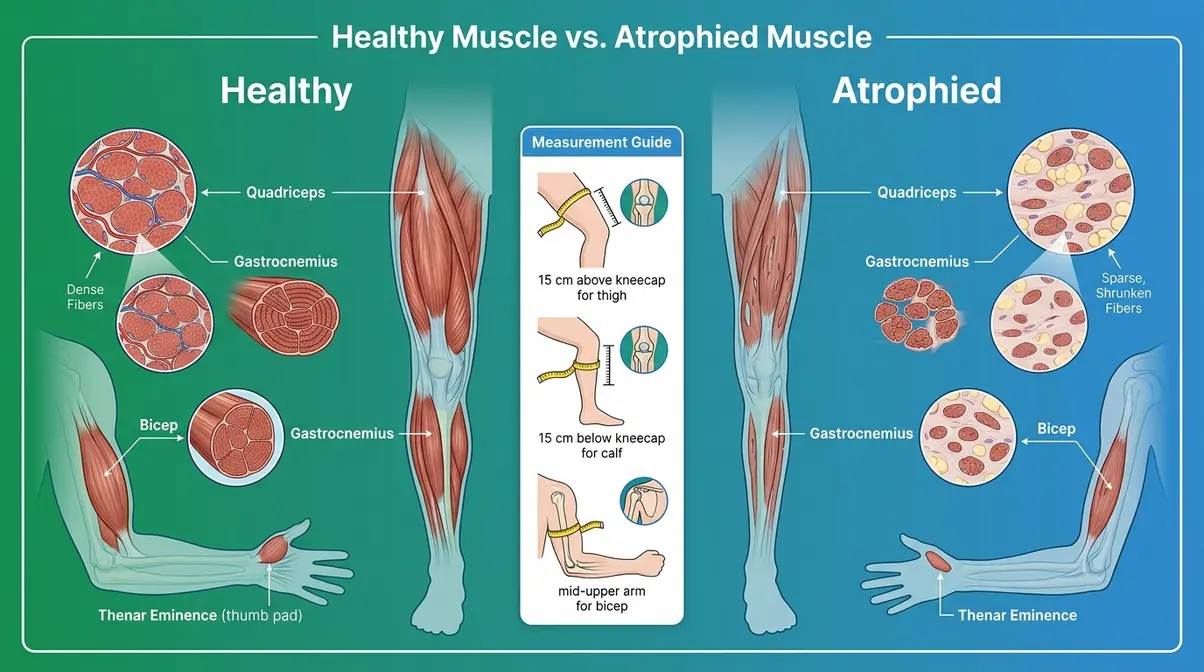
The lower body is the most commonly affected region in both disuse and age-related atrophy. The quadriceps (front of the thigh), hamstrings (back of the thigh), and gastrocnemius (calf muscle) are particularly vulnerable because they are large, weight-bearing muscles that atrophy rapidly when walking and standing are reduced.
- Signs specific to leg muscle atrophy:
- One thigh or calf visibly thinner than the other (measure with a tape measure 15 cm above or below the kneecap for objective comparison)
- Difficulty rising from a low chair without using your hands
- Knee instability or “giving way” during walking
- Calf atrophy often presents as difficulty standing on tiptoe or pushing off during walking
- Targeted exercises for leg atrophy:
- Straight leg raises: Lying flat, tighten one quadricep and lift the straight leg to 45°. Hold 3 seconds, lower. 3 × 15 reps.
- Seated knee extensions: Sitting in a chair, slowly extend one knee to straight. 3 × 12 reps.
- Standing calf raises: Behind a chair for balance, rise onto toes, lower slowly. 3 × 15 reps.
- Step-ups: Step onto a low step (6–8 inches), lead with the weaker leg. 3 × 10 reps each side.
Physical therapists consistently recommend beginning lower-body atrophy rehabilitation with seated exercises before progressing to standing weight-bearing exercises — this protects joints while rebuilding foundational strength.
Hand, Arm, and Thenar Atrophy
Upper-limb atrophy is less common from disuse alone but is frequently seen after arm fractures, rotator cuff repairs, or in neurological conditions affecting the cervical spine (neck) or peripheral nerves.
Thenar muscle atrophy (wasting of the fleshy pad at the base of the thumb) is a hallmark sign of carpal tunnel syndrome (compression of the median nerve at the wrist). If you notice the thumb-side of your palm looking flattened or hollow, this warrants prompt medical evaluation — it indicates significant nerve compression that may require surgical intervention.
- Signs of arm and hand atrophy:
- Visible thinning of the forearm or upper arm
- Weakened grip strength — difficulty opening jars, turning keys, or holding objects
- Reduced pinch strength in the thumb and index finger
- Thenar eminence (thumb pad) appears flat compared to the other hand
- Targeted exercises for arm and hand atrophy:
- Grip strengthening: Squeeze a soft rubber ball or therapy putty for 5 seconds, release. 3 × 15 reps.
- Wrist curls: Light dumbbell (0.5–1 kg), palm up, curl wrist upward. 3 × 12 reps.
- Bicep curls with resistance band: Anchor band underfoot, curl hand toward shoulder. 3 × 12 reps.
- Shoulder external rotation: Resistance band anchored at elbow height, rotate forearm outward. 3 × 12 reps.
Neurogenic and Pathologic Atrophy
Neurogenic and pathologic atrophy represent the more severe end of the muscle atrophy spectrum. While disuse atrophy is largely a mechanical problem with a mechanical solution, these forms involve underlying biological disruptions that require specialized medical management.
Understanding Neurogenic Atrophy
Neurogenic atrophy (muscle loss caused by nerve damage) occurs when the motor nerve supplying a muscle is injured, compressed, or destroyed. Without a functioning nerve signal, the muscle loses both its ability to contract and its primary trophic (growth-maintaining) stimulus. The result is rapid, severe wasting — often faster and more extensive than disuse atrophy.
Key conditions associated with neurogenic atrophy include:
- ALS (amyotrophic lateral sclerosis): A progressive neurodegenerative disease that destroys motor neurons throughout the body, causing progressive muscle atrophy that eventually affects breathing and swallowing. The Muscular Dystrophy Association (MDA) notes that ALS affects approximately 30,000 Americans at any given time.
- Spinal cord injury: Damage to the spinal cord disrupts nerve signals below the injury level, causing immediate and severe atrophy in the affected muscles.
- Peripheral neuropathy: Damage to peripheral nerves (often from diabetes, alcohol use, or autoimmune disease) causes gradual, distal (extremity-first) atrophy — typically beginning in the feet and hands.
- Brachial plexus injury: Damage to the nerve network serving the arm and shoulder, often from trauma, causes rapid upper-limb atrophy.
- Progressive muscular atrophy (PMA): A rare variant of motor neuron disease causing selective lower motor neuron degeneration and progressive limb wasting.
Neurogenic atrophy requires prompt diagnosis by a neurologist. Treatment focuses on managing the underlying condition, protecting remaining nerve function, and using NMES and passive exercise to maintain muscle bulk where voluntary contraction is impossible.
ICD-10 Medical Codes
For healthcare providers, caregivers, and patients navigating insurance or medical records, muscle atrophy has specific ICD-10-CM (International Classification of Diseases, 10th Revision) codes:
| Condition | ICD-10 Code |
|---|---|
| Muscle wasting and atrophy, not elsewhere classified | M62.50 |
| Muscle wasting — upper arm | M62.521/M62.522 |
| Muscle wasting — lower leg | M62.561/M62.562 |
| Paraspinal muscle atrophy | M62.58 |
| Multifidus muscle atrophy | M62.58 (same category) |
| Neurogenic muscular atrophy | G12.29 (motor neuron disease) |
| Disuse atrophy (specified site) | M62.5– (site-specific) |
Paraspinal muscle atrophy (wasting of the muscles running alongside the spine) and multifidus muscle atrophy (wasting of the deep spinal stabilizer muscle) are increasingly recognized as contributors to chronic low back pain and spinal instability. MRI studies show that multifidus atrophy is present in a high percentage of patients with chronic low back pain — and targeted rehabilitation of this muscle is a primary goal of modern physical therapy for back pain.
Muscle Atrophy in Pets
Muscle atrophy is not exclusive to humans. Dogs and cats experience the same biological process — and pet owners who notice visible muscle loss in their animals are right to be concerned. Early veterinary intervention follows the same principles as human care: identify the cause, address it medically, and implement a structured rehabilitation plan.
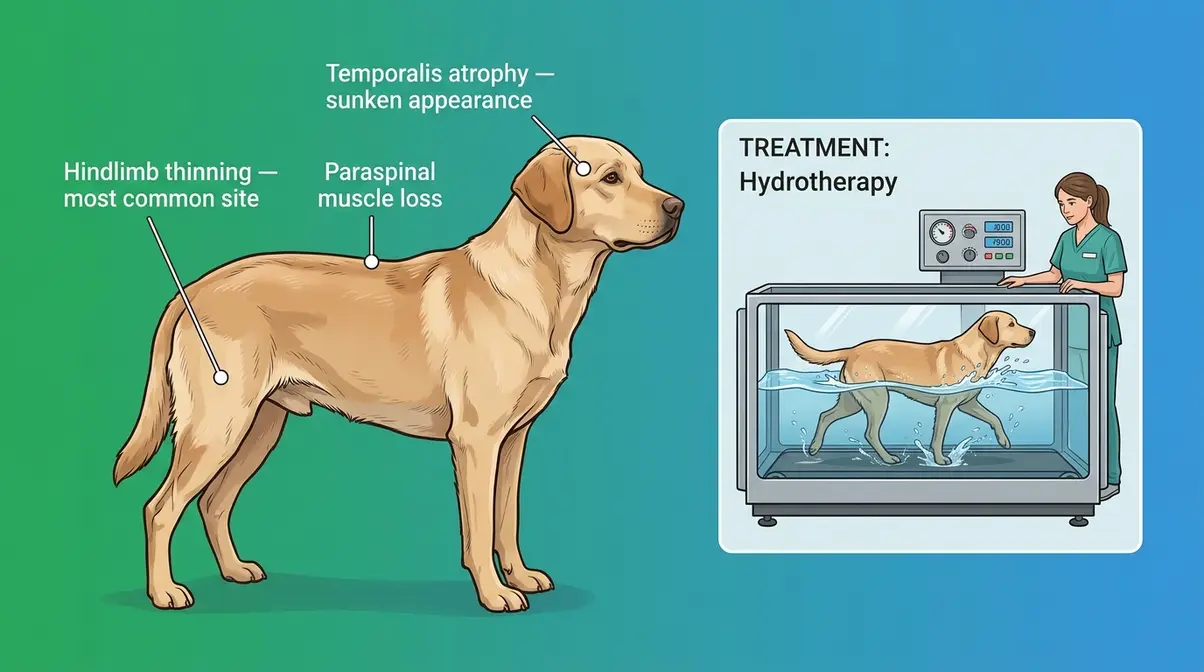
Signs of Atrophy in Dogs
Canine muscle atrophy most commonly affects the hindquarters (back legs and hips), the temporalis muscles of the skull (giving the head a sunken appearance), and the spine. According to veterinary clinical guidelines, the most common causes in dogs include:
- Orthopedic conditions: Hip dysplasia, cruciate ligament tears, and arthritis cause disuse atrophy in the affected limb as the dog avoids bearing weight
- Neurological conditions: Degenerative myelopathy (similar to ALS in humans), intervertebral disc disease (IVDD), and peripheral neuropathy
- Systemic illness: Cancer, Cushing’s disease (hyperadrenocorticism), and severe chronic illness can cause generalized muscle wasting
- Age-related sarcopenia: Senior dogs (typically over 8–10 years, depending on breed) experience progressive muscle loss similar to human aging
- Warning signs in dogs:
- Visible thinning of the thighs or hindquarters; dog “bunny hops” rather than walking normally
- Skull appears sunken or “bony” around the temples (temporalis atrophy — often a sign of masticatory muscle myositis, an autoimmune condition)
- Reluctance to climb stairs, jump, or rise from lying down
- Noticeable difference in muscle bulk between left and right hindlimbs
If you notice any of these signs, schedule a veterinary examination promptly. Neurological causes in particular progress rapidly and require urgent diagnosis.
Veterinary Care for Pets
Veterinary treatment of muscle atrophy mirrors the human approach — address the underlying cause first, then implement rehabilitation.
- Veterinary diagnostic workup typically includes:
- Physical examination and orthopedic/neurological assessment
- X-rays of affected joints or spine
- Blood panel (checking for metabolic and endocrine causes)
- MRI or CT scan for neurological cases
Treatment options for canine and feline atrophy:
- Controlled exercise rehabilitation: Veterinary physiotherapists use underwater treadmill therapy (hydrotherapy) as a primary tool — the buoyancy of water allows the dog to exercise the atrophied muscles without bearing full body weight, reducing pain and risk of injury.
- Nutritional support: High-quality, protein-rich diets are recommended for dogs recovering from atrophy. Veterinary nutritionists may recommend therapeutic diets or protein supplementation.
- Pain management: For orthopedic causes, managing pain with NSAIDs (non-steroidal anti-inflammatory drugs, prescribed by a vet) reduces the dog’s reluctance to use the affected limb — which in turn reduces disuse atrophy.
- NMES and laser therapy: Some veterinary rehabilitation centers use neuromuscular electrical stimulation and low-level laser therapy to stimulate atrophied muscles, particularly in dogs with spinal cord disease.
- Surgical intervention: For cruciate ligament tears or severe disc disease, surgery followed by structured rehabilitation is often the most effective path to recovery.
For cats, muscle atrophy most commonly presents in older animals with hyperthyroidism (overactive thyroid — one of the most common feline endocrine disorders) or chronic kidney disease. Medical management of the underlying condition, combined with high-protein dietary support, is the primary treatment approach.
Limitations & When to See a Doctor
Common Mistakes in Recovery
Physical therapists and rehabilitation specialists consistently identify these as the most common — and most consequential — errors people make when trying to recover from muscle atrophy:
- Starting too intensely, too fast. Atrophied muscle tissue is fragile. Jumping straight into heavy resistance training without progressing through the earlier stages (isometric → bodyweight → resistance) significantly increases injury risk and can set recovery back by weeks.
- Ignoring nutrition. Exercise without adequate protein is like building a house without materials. Many people focus entirely on exercise while eating insufficient protein — and then wonder why their strength isn’t returning. Meet your protein targets first.
- Stopping rehabilitation when “it feels better.” Muscle bulk and strength return at different rates. You may feel functional improvement weeks before full muscle mass is restored. Stopping too early leaves residual atrophy that increases the risk of re-injury.
- Self-diagnosing neurogenic atrophy as disuse atrophy. If your muscle loss is accompanied by numbness, tingling, or pain, it is not simple disuse atrophy. Treating neurogenic atrophy with exercise alone — without addressing the underlying nerve problem — will not produce meaningful recovery.
When to See a Doctor Immediately
Seek medical attention promptly if you experience:
- Sudden, rapid muscle loss — particularly if it affects both sides of your body symmetrically
- Muscle weakness with neurological symptoms — numbness, tingling, burning, or loss of bladder/bowel control
- Difficulty swallowing or breathing alongside muscle weakness (a potential sign of ALS or myasthenia gravis)
- Visible muscle wasting in a child — pediatric muscle atrophy is always a red flag requiring urgent evaluation
- Atrophy following a period of severe illness, high fever, or ICU admission — intensive care unit-acquired weakness (ICUAW) is a serious and underrecognized condition
- No improvement after 4–6 weeks of consistent structured rehabilitation
The general rule: if your atrophy has a clear, obvious cause (a broken bone in a cast, planned bed rest) and is improving with rehabilitation, monitor and continue treatment. If the cause is unclear, the atrophy is progressing despite treatment, or you have any neurological symptoms — see a doctor.
Conditions That Mimic Atrophy
Not all apparent muscle loss is true atrophy. Conditions that can look like atrophy include:
- Edema resolution — when significant swelling (edema) resolves, the limb may appear to have “lost muscle” but the change is actually loss of fluid
- Lipodystrophy — selective loss of subcutaneous fat (not muscle) can give the appearance of muscle wasting
- Severe dehydration — can temporarily reduce muscle volume without true fiber atrophy
A proper medical evaluation distinguishes true atrophy from these mimics.
Frequently Asked Questions About Muscle Atrophy
How do you treat atrophy?
Muscle atrophy treatment combines progressive resistance exercise with adequate protein intake — this dual approach is the evidence-based standard of care. Begin with isometric contractions and range-of-motion exercises, then progress to bodyweight and resistance training over 4–8 weeks. Protein intake should reach 1.2–2.0 g/kg body weight daily depending on age and severity. For neurogenic or disease-related atrophy, treatment of the underlying cause must come first, often under the supervision of a neurologist and physical therapist. Always consult a licensed DPT before beginning a rehabilitation program.
What is the fastest way to build atrophied muscle?
The fastest way to build atrophied muscle is by combining progressive resistance training with a high-protein diet (1.6–2.0 g/kg of body weight). Acting within the first 4–6 weeks—known as The Rebuild Window—takes advantage of muscle memory to accelerate recovery. Ensure you distribute protein evenly across 4 meals and time intake around your workouts to maximize muscle protein synthesis.
Does walking help reverse muscle atrophy?
Yes, walking is an excellent starting point for reversing mild disuse atrophy in the legs. It provides a foundational mechanical stimulus and improves blood flow to the recovering tissues. However, to fully rebuild muscle mass and strength, you will eventually need to introduce progressive resistance exercises like squats, step-ups, or resistance band work to challenge the muscle fibers adequately.
What are the first signs of muscle atrophy?
The first signs of muscle atrophy include visible thinning of a limb, reduced grip or lifting strength, and increased fatigue during routine activities. You may notice that one arm or leg looks noticeably smaller than the other, that clothing fits differently, or that tasks you previously managed easily — climbing stairs, rising from a chair — now require noticeably more effort. Neurogenic atrophy may additionally cause tingling, numbness, or muscle twitching in the affected area. Catching these signs early — ideally within the first 2–3 weeks — significantly shortens recovery time.
Can muscle atrophy be reversed?
Muscle atrophy can be reversed in most cases, especially disuse atrophy. The key variables are: how long the atrophy has been present, the underlying cause, the individual’s age, and how quickly structured rehabilitation begins. A 2016 study in the Journal of Experimental Biology (Gundersen) showed that muscles rebuild 2–3 times faster in previously trained individuals due to retained myonuclei — a phenomenon that supports aggressive early rehabilitation. Neurogenic and severe pathologic atrophy may only be partially reversible, depending on the extent of nerve or systemic damage. Consult a DPT and physician for a personalized prognosis.
Is muscle atrophy dangerous?
Muscle atrophy can be dangerous when left untreated, particularly in older adults and those with underlying neurological conditions. In older adults, significant muscle loss increases fall risk by up to 60% and is strongly associated with fractures, hospitalization, and reduced lifespan (Frontera & Ochala, Physiological Reviews, 2015). In neurogenic forms, progressive atrophy can impair breathing and swallowing. However, disuse atrophy in otherwise healthy individuals — while serious — responds well to treatment and rarely poses a life-threatening risk on its own. The danger lies primarily in delayed treatment and the downstream consequences of prolonged weakness.
Reversing Muscle Atrophy: Your Action Plan
Muscle atrophy is one of the most common — and most treatable — conditions affecting the human body. The biology is clear: without consistent mechanical stimulus and adequate nutritional support, muscle tissue shrinks. With the right rehabilitation approach, most of that lost muscle can be rebuilt.
Here’s what the evidence shows, distilled to its essentials: muscle atrophy causes measurable loss within days, becomes visible within weeks, and responds to structured treatment within weeks to months — depending on how quickly you act. Research consistently confirms that acting within The Rebuild Window (the first 4–6 weeks after onset) is the single most powerful predictor of full recovery. Retained myonuclei give your body a biological head start that makes early action exponentially more effective than delayed action.
The framework is straightforward: progress through the 6-step exercise protocol from isometric contractions to functional training, meet your daily protein target (1.2–2.0 g/kg depending on your age and severity), and consult a physical therapist for hands-on guidance. For neurogenic or pathologic atrophy, see a specialist before beginning any exercise program — treating the underlying cause is the first step.
Your next step: schedule an appointment with a licensed physical therapist (DPT) this week. Bring a written record of when you first noticed symptoms, which muscles are affected, and any relevant medical history. The sooner you begin, the shorter your road back to full strength.
Related posts:
What Is Muscle Memory? The Complete Science Guide
Muscle Hypertrophy Explained: The Science of Muscle Growth
Strength Training vs Hypertrophy: The Complete 2026 Guide
Muscle Building Transformation Stories: What Actually Worked
How Many Sets and Reps for Strength Training? Chart by Goal
Muscles Used in Rock Climbing: All 20+, Not Just Forearms
Callum
Hi, I'm Callum, the founder of Body Muscle Matters. I'm not a certified trainer, I'm a self taught lifter who started this site to share what I've learned from my own training and a lot of trial and error. Everything here comes from real experience and honest research, written the way I'd explain it to a friend who is just getting started. My goal is simple: practical, no hype fitness advice you can actually use.