
Most women consume around 70 grams of protein per day — but depending on your body weight, age, and goals, your body may need up to 130g or more. That gap isn’t trivial. It’s the difference between a metabolism that hums along and one that stalls, between muscles that recover and ones that slowly diminish, between feeling strong at 55 and feeling exhausted and stiff.
If you’ve been eating “healthy” but still struggle with low energy, stubborn weight, or poor muscle tone despite working out, your protein intake for women may be the variable you’ve been overlooking all along. Under-eating protein doesn’t just limit muscle — it disrupts satiety, slows metabolism, and accelerates the muscle loss that begins quietly in your 30s and loudly in your 50s.
By the end of this guide, you’ll know your exact daily protein target — calculated from your weight and your goal — so you can stop guessing and start making measurable progress. We’ll walk through a step-by-step framework covering daily calculation, life-stage adjustments (including perimenopause and pregnancy), food sources, and the kidney safety question that stops many women from eating enough protein.
Most women need 1.2–2.0g of protein per kilogram of body weight daily — significantly more than the government’s 0.8g/kg survival minimum. The Thriving Threshold Framework presented in this guide gives you a personalized target based on your weight, goal, and life stage, so you can move from surviving to genuinely thriving.
- The 0.8g/kg RDA is a floor, not a goal: Research consistently supports 1.2–2.0g/kg for active women and those over 40.
- The Leucine Threshold matters: Aim for 30g of high-quality protein per meal to trigger muscle repair and growth at the cellular level.
- Life stage changes everything: Perimenopausal and postmenopausal women need 1.6–2.0g/kg — often double what most eat.
- Protein is safe for healthy kidneys: Concerns are specific to women with diagnosed kidney disease, not the general population.
Stop treating protein as a gym concept — it’s a foundational tool for every life stage.
- 1. Calculate your personal g/kg target this week — don’t estimate; your actual body weight determines your actual number.
- 2. Restructure meals around a 30g protein anchor — implement the leucine threshold at breakfast first, as it’s the meal most women underdeliver.
- 3. If you’re 40+, increase your target to 1.6–2.0g/kg — and pair it with strength training at least twice a week to overcome anabolic resistance.
Before You Start — Protein Intake Basics
Before you pick up a calculator, it helps to understand why protein matters so much for women specifically. This section covers the foundation — what protein actually does in your body, and what the terms in this guide mean. If you already know what RDA and g/kg mean, feel free to skip to Step 1.
What Is Protein? The Macronutrient Your Body Can’t Build Without
Protein is one of three macronutrients (the others being carbohydrates and fat) — meaning your body needs it in large amounts to function. Unlike carbohydrates and fat, however, protein isn’t primarily an energy source. It’s a builder and repairer.
Every cell in your body contains protein. Your muscles, skin, hair, nails, hormones, enzymes, and immune system antibodies are all made from protein. When you eat protein-rich food, your digestive system breaks it down into smaller units called amino acids (the individual building blocks). Your body then uses those amino acids to repair damaged muscle tissue, create new muscle, produce hormones like estrogen and insulin, support immune function, and maintain the lean muscle mass that drives your metabolism (the rate at which your body burns calories at rest).
For women specifically, adequate protein supports hormonal balance, bone density, and the preservation of lean muscle mass — the metabolically active tissue that declines with age if protein intake doesn’t compensate. This decline has a name: sarcopenia (age-related muscle loss that accelerates after 50), and it is not inevitable if you eat enough protein combined with regular movement.
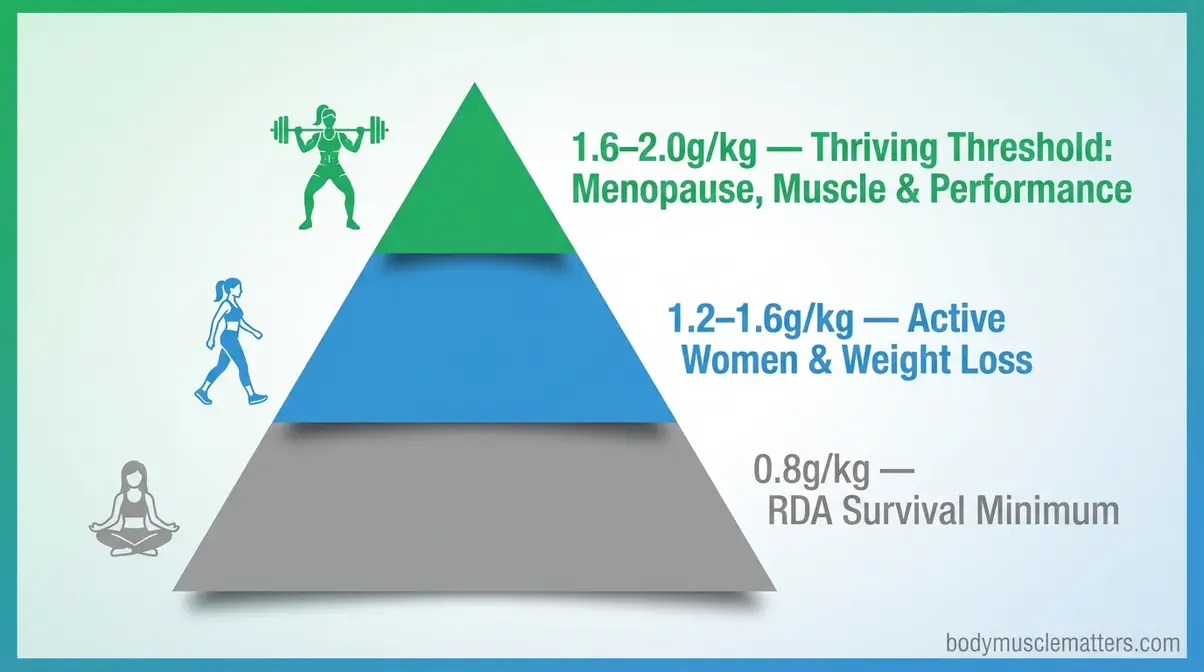
Caption: The RDA of 0.8g/kg represents a survival minimum — the Thriving Threshold Framework targets the upper evidence-based range of 1.2–2.0g/kg.
Key Terms You’ll See in This Guide
Understanding these terms now will make every calculation step feel straightforward.
| Term | What It Means |
|---|---|
| RDA (Recommended Dietary Allowance) | The government’s minimum daily target — the amount needed to prevent deficiency in most healthy adults. For protein, it’s 0.8g/kg. It is NOT an optimal target. |
| g/kg | Grams per kilogram of body weight. Your target is expressed this way so it scales to your actual body size. |
| Lean body mass | Your body weight minus fat. Some advanced calculations use this instead of total weight. |
| Leucine threshold | The minimum amount of the amino acid leucine needed per meal to trigger muscle protein synthesis (repair and building). |
| Sarcopenia | Age-related muscle loss. Begins gradually in your 30s, accelerates after 50. Protein + resistance exercise are the two most evidence-based ways to slow it. |
| Anabolic resistance | The reduced ability of aging muscle to respond to protein. It means older women need more protein per meal, not less, to get the same muscle-building signal. |
| TEF (Thermic Effect of Food) | The calories your body burns digesting food. Protein has the highest TEF at 20–30%, compared to 5–10% for carbs. |
| MPS (Muscle Protein Synthesis) | The cellular process by which your body builds new muscle protein. The goal of strategic protein intake is to stimulate MPS multiple times per day. |
Step 1 — Calculate Your Daily Protein Intake as a Woman
This step gives you a precise personal number. The step-by-step calculation method in this guide is based on the ISSN’s position stand on protein and exercise, cross-referenced with NIH research on older women’s needs. The six subsections below build on each other — read them in order.
Why the 0.8g/kg RDA Isn’t Enough for Most Women
The RDA for protein is 0.8 grams per kilogram of body weight — a number set by the Institute of Medicine as the minimum needed to prevent muscle breakdown in a sedentary adult. For a 68kg (150lb) woman, that’s just 54 grams per day.
Here’s the critical distinction most health websites miss: the RDA was designed to prevent deficiency in a sedentary population under controlled conditions. It was never intended as a target for optimal health, weight management, or muscle preservation. Registered dietitians widely recognize this gap, and subsequent research has consistently shown that women who eat only 0.8g/kg lose more muscle during calorie deficits, have weaker satiety signals, and experience faster age-related muscle decline than women eating 1.2g/kg or higher (Stanford Lifestyle Medicine, 2024).
The difference in practice is significant. At 0.8g/kg, a 68kg woman eats 54g of protein per day — roughly two chicken breasts. At 1.6g/kg, the same woman eats 109g — a target that most dietitians consider the starting point for active or midlife women. The Thriving Threshold Framework used throughout this guide draws a clear line between surviving (0.8g/kg) and thriving (1.2–2.0g/kg), based on your goal and life stage.
Individual needs vary. Consult a registered dietitian or your doctor before significantly changing your protein intake.
Harvard Health explains that while the RDA is 0.8g/kg, many experts consider this a floor — not a ceiling.
The Optimal Range: 1.2–2.0g/kg Explained
For most women, the evidence-based optimal range is 1.2–2.0g/kg of body weight per day, depending on activity level, age, and goal. Here is how that range breaks down by category:
| Goal / Life Stage | Protein Target (g/kg) | Example: 68kg Woman |
|---|---|---|
| Sedentary, general health maintenance | 1.0–1.2g/kg | 68–82g/day |
| Active, weight loss | 1.2–1.6g/kg | 82–109g/day |
| Active, muscle building | 1.6–2.2g/kg | 109–150g/day |
| Perimenopause / ages 45–55 | 1.6–2.0g/kg | 109–136g/day |
| Postmenopause / ages 55+ | 1.6–2.0g/kg | 109–136g/day |
| Pregnant (2nd/3rd trimester) | 1.1g/kg + 25g/day | ~100–110g/day |
| Breastfeeding | +25g over baseline | ~95–125g/day |
These numbers reflect current clinical consensus from sources including UCLA Health and Stanford Lifestyle Medicine (2024), which recommend 1.2–1.6g/kg for adults over 50 as a baseline protective minimum.
How to Use the g/kg Formula: A Step-by-Step Calculation
You’ll need your weight in kilograms. If you only know your weight in pounds, divide by 2.2. If you’re unsure where to start, you can verify your calculation with our guide on how to calculate your exact daily protein needs.
- Step 1: Convert your weight to kilograms.
- Weight in pounds ÷ 2.2 = weight in kg
- Example: 150 lbs ÷ 2.2 = 68 kg
- Step 2: Choose your protein multiplier from the table above.
- Example: Active woman focused on weight loss → 1.4g/kg
- Step 3: Multiply.
- Weight in kg × protein multiplier = daily protein target in grams
- Example: 68 kg × 1.4 = 95g of protein per day
- Step 4: Divide across your meals.
- Daily target ÷ number of meals = protein per meal
- Example: 95g ÷ 3 meals = ~32g per meal
Worked example at each life stage for a 68kg woman:
| Life Stage | Multiplier | Daily Target | Per Meal (3 meals) |
|---|---|---|---|
| Ages 25–35, active | 1.4g/kg | 95g | ~32g |
| Perimenopause, 45–55 | 1.8g/kg | 122g | ~41g |
| Postmenopause, 55+ | 2.0g/kg | 136g | ~45g |
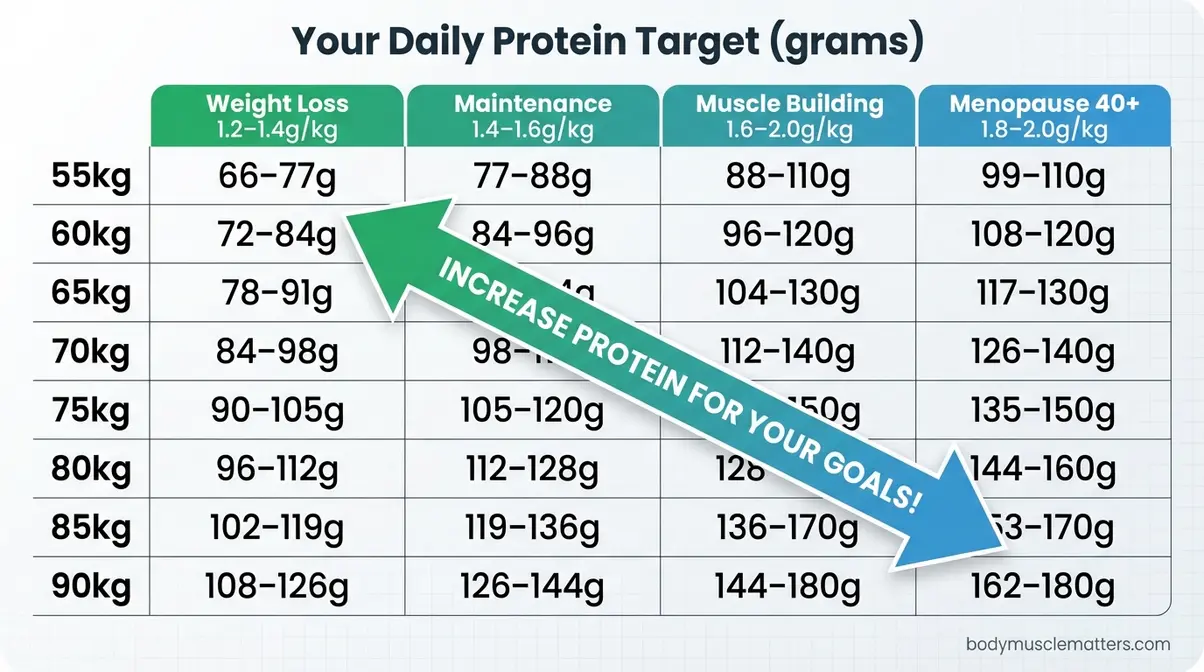
Caption: Use this matrix to find your personal protein target in seconds — cross-reference your weight row with your goal column.
The Leucine Threshold: Why 30g Per Meal Is the Trigger
Not all protein you eat ends up building muscle. Your body only activates muscle protein synthesis (the repair and growth process) when a specific amino acid — leucine — reaches a threshold concentration in your bloodstream.
Research confirms that older adults need to reach a “meal threshold” for leucine to trigger the mTORC1 signaling pathway — the cellular switch that tells muscle tissue to rebuild. For younger women, that threshold is typically reached with approximately 2.5g of leucine per meal, which is contained in roughly 25–30g of high-quality animal protein (such as chicken, eggs, or Greek yogurt). For women over 40 — due to anabolic resistance — that threshold rises to approximately 2.5–3g of leucine per meal, often requiring closer to 30–40g of protein to achieve the same effect.
In practical terms: eating 30g of protein at a meal is the trigger, not just a target. Below this amount, you get some benefit — but you don’t maximally stimulate the repair process your muscles need. This is why spreading your daily total across three or four meals is far more effective than eating 20g at breakfast and 70g at dinner.
“Recommend 4 or more daily meals or snacks with high protein (20–40g) and a total intake of 120g (low side) to 160g (high side).”
This advice — common among sports dietitians working with active women — reflects the science of the leucine threshold. Four meals at 30–40g each hits both the daily total and the per-meal trigger.
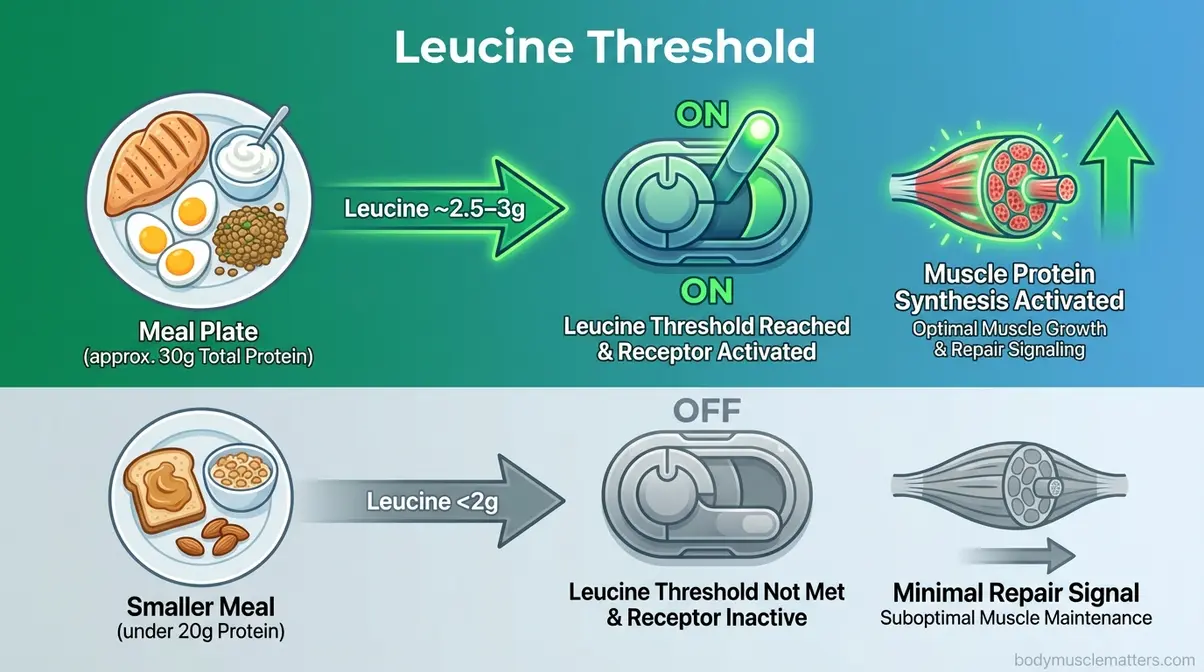
Caption: The leucine threshold is the cellular “on switch” for muscle repair — each meal needs to cross it to count.
Protein Distribution: Spreading Your Daily Total Across Meals
How you distribute protein across the day matters nearly as much as your total. Research on protein distribution consistently shows that evenly spreading intake across three to four meals produces significantly better muscle protein synthesis outcomes than front- or back-loading.
The most common mistake women make is eating a low-protein breakfast (toast, coffee, maybe yogurt), a moderate-protein lunch, and then eating 50–60g of protein at dinner. This pattern fails the leucine threshold test at breakfast and lunch — two out of three meals don’t trigger meaningful muscle repair. Here is a more effective distribution model:
- Recommended daily distribution for a 95g target (3 meals + 1 snack):
- Breakfast: 30g protein
- Lunch: 30g protein
- Afternoon snack: 15g protein
- Dinner: 20g protein
- Total: 95g
For women who fast (intermittent fasting): A 2023 analysis of protein timing and cortisol suggests that breaking a fast with a complete protein source (at least 30g, leucine-rich) minimizes muscle catabolism (breakdown) that accumulates overnight. Skipping protein at your first meal of the day — even if that meal is at noon — means your muscle tissue has been in a breakdown state for 16+ hours with no repair signal. Break your fast with eggs, Greek yogurt with protein powder, or a high-protein smoothie.
Your Quick-Reference Protein Target Chart
Use this chart to find your daily protein target based on body weight and goal. All targets reflect the Thriving Threshold Framework’s 1.2–2.0g/kg range.
| Body Weight | Weight Loss (1.2–1.4g/kg) | Maintenance (1.4–1.6g/kg) | Muscle Building (1.6–2.0g/kg) | Menopause/40+ (1.8–2.0g/kg) |
|---|---|---|---|---|
| 55 kg (121 lbs) | 66–77g | 77–88g | 88–110g | 99–110g |
| 60 kg (132 lbs) | 72–84g | 84–96g | 96–120g | 108–120g |
| 68 kg (150 lbs) | 82–95g | 95–109g | 109–136g | 122–136g |
| 75 kg (165 lbs) | 90–105g | 105–120g | 120–150g | 135–150g |
| 82 kg (180 lbs) | 98–115g | 115–131g | 131–164g | 148–164g |
| 90 kg (198 lbs) | 108–126g | 126–144g | 144–180g | 162–180g |
Individual needs vary. Consult a registered dietitian or your doctor before significantly changing your protein intake.
Step 2 — Adjust Your Protein Intake for Weight Loss

Protein is the most powerful macronutrient for weight loss — not because it’s “magic,” but because of three measurable biological mechanisms. Our review of current nutrition research shows that women who hit their protein target during a calorie deficit preserve more muscle, feel fuller longer, and burn more calories passively than those who cut calories without adjusting protein. For a detailed breakdown of specific foods to prioritize, review our guide on the best protein strategy for weight loss.
How Protein Boosts Your Metabolism (The Thermic Effect of Food)
The Thermic Effect of Food (TEF) is the number of calories your body burns simply digesting and processing what you eat. Protein has a TEF of 20–30%, meaning for every 100 calories of protein you consume, your body burns 20–30 calories just to break it down. Carbohydrates have a TEF of 5–10%, and fat has a TEF of just 0–3%.
In practical terms: if you eat 120g of protein per day (approximately 480 calories from protein), your body burns roughly 96–144 of those calories through digestion alone. That’s a meaningful metabolic advantage that compounds over weeks and months of consistent intake. This mechanism partly explains why research supports higher-protein diets for women during calorie deficits — they produce greater fat loss relative to muscle loss compared to standard-protein diets (Mayo Clinic Health System, 2024).
Mayo Clinic Health System confirms that while protein is crucial, balance is key — but the thermic advantage remains a distinct benefit for weight management.
Preventing Lean Muscle Loss During a Calorie Deficit
The single biggest risk of a calorie deficit without adequate protein is lean muscle loss. When you eat fewer calories than you burn, your body needs energy from somewhere. Without sufficient protein, it turns to muscle tissue — breaking down your metabolically active lean mass to fuel basic functions. This is called catabolism, and it’s the reason many women who “diet” end up lighter but flabbier, with a slower metabolism than before.
Research consistently shows that women eating 1.2–1.6g/kg of protein during a calorie deficit preserve significantly more lean muscle mass than those eating at the 0.8g/kg RDA level. Preserving muscle during weight loss matters for three reasons:
- Muscle burns more calories at rest than fat tissue — losing it slows your metabolism permanently.
- Muscle gives your body shape and tone — the “toned” look most women want comes from muscle visibility, not just fat loss.
- Muscle protects your joints and improves physical function — especially important for women entering their 40s and 50s.
Your Weight Loss Protein Target: The 1.2–1.6g/kg Range
During a calorie deficit, aim for 1.2–1.6g/kg of body weight per day as your protein floor. If you are exercising four or more days per week, target the higher end of this range (1.5–1.6g/kg) to compensate for the increased muscle breakdown that exercise itself creates.
- Worked example: A 68kg woman on a weight loss program
- Conservative target (1.2g/kg): 82g/day
- Active target (1.6g/kg): 109g/day
- Recommended approach: Start at 1.4g/kg (95g/day) and adjust based on energy, recovery, and satiety
Individual needs vary. Consult a registered dietitian or your doctor before significantly changing your protein intake.
Sample High-Protein Day for Weight Loss
Here is a practical example of a 95g protein day built around whole foods, designed for a woman on a moderate calorie deficit (~1,500–1,800 kcal):
| Meal | Food | Protein |
|---|---|---|
| Breakfast | 2 eggs + 150g Greek yogurt (0% fat) + ½ cup berries | ~30g |
| Lunch | 120g grilled chicken breast + large salad + lentils (½ cup) | ~35g |
| Snack | 30g almonds + 1 low-fat string cheese | ~10g |
| Dinner | 100g salmon + roasted vegetables + ½ cup quinoa | ~30g |
| Total | ~105g |
This structure hits the leucine threshold at breakfast and lunch (≥30g), provides fiber-rich carbohydrates for energy, and keeps total calories within a deficit range. The satiety (feeling of fullness) benefit of protein is well documented — high-protein meals significantly reduce hunger hormones like ghrelin, making calorie restriction far easier to sustain.
Special Case: Protein for Women on GLP-1 Medications (Ozempic/Wegovy)
GLP-1 medications (semaglutide, tirzepatide) suppress appetite so effectively that many women inadvertently under-eat protein — at the exact time they most need it. Recent findings in JAMA Network Open highlight that while these medications drive significant weight loss, preserving lean mass requires a dedicated nutritional strategy. The so-called “Ozempic Face” or “Ozempic Body” often reflects rapid loss of lean tissue alongside fat.
Research suggests that without intervention, a significant portion of weight lost on GLP-1 medications may come from lean muscle mass — a serious long-term metabolic risk. To counter this, clinical guidance increasingly points toward higher protein targets combined with resistance training.
- GLP-1 Protein Protocol:
- Target 1.6–2.0g/kg of body weight in protein daily — the higher end of the therapeutic range to counteract catabolic effects.
- Prioritize protein at every meal, even if appetite is suppressed. If eating a full meal feels difficult, start with the protein portion first.
- Use protein-rich snacks (Greek yogurt, cottage cheese, hard-boiled eggs) between meals to maintain daily totals.
- Pair protein intake with resistance training at least 2–3 times per week — medication alone does not prevent muscle loss; the protein-exercise combination is essential.
If you are on GLP-1 medications, discuss specific protein targets with your prescribing physician or a registered dietitian, as individual needs vary significantly.
Step 3 — Optimize Your Protein Intake to Build Lean Muscle

Building lean muscle as a woman is both more achievable and more important than most popular media suggests. The limiting factor for most women isn’t their workout routine — it’s chronically under-eating protein. After reviewing current nutrition research, the picture is clear: women who hit 1.6–2.2g/kg daily, combined with progressive resistance training, consistently build meaningful muscle without becoming “bulky.” For a deeper dive into specific muscle-building protocols, read our full guide on protein targets for building lean muscle.
Busting the ‘Bulky’ Myth: What Protein Actually Does to Women’s Muscles
High protein intake does not make women “bulky.” This is one of the most persistent and damaging myths in women’s fitness. The “bulky” physique associated with bodybuilders results from years of extremely high-volume training, specific genetic factors, and in many cases, performance-enhancing substances — not from eating 120g of protein per day.
What adequate protein actually does for women’s muscles is this: it repairs the micro-tears created by exercise, gradually increasing muscle fiber diameter (called hypertrophy) over months. For most women, this process produces lean, defined muscles — not large, bulging ones. Women produce roughly 15–20 times less testosterone than men, which is the primary hormonal driver of significant muscle mass in male bodybuilders. Higher protein intake, combined with resistance exercise, helps women achieve a leaner body composition with better metabolic function — exactly what most women training for health and aesthetics actually want.
The 1.6–2.2g/kg Target for Active Women: What the Research Says
For women actively training to build muscle, the evidence-based target is 1.6–2.2g/kg of body weight per day. The International Society of Sports Nutrition (ISSN) Position Stand on nutritional concerns of the female athlete specifically recommends that daily protein intake should fall within 1.4–2.2g/kg for women engaged in resistance training.
Importantly, the ISSN notes that requirements may shift during your menstrual cycle. During the luteal phase (the week before your period), progesterone’s catabolic effects may increase protein breakdown, meaning you should aim for the upper end of your range to maintain recovery.
- Worked example for a 68kg woman building muscle:
- Maintenance Training: 1.4–1.6g/kg (95–109g/day)
- Hypertrophy Phase: 1.6–2.0g/kg (109–136g/day)
- High-Volume / Luteal Phase: 2.0–2.2g/kg (136–150g/day)
The upper range (2.0–2.2g/kg) is generally reserved for women in high-volume training phases (5+ days/week), women over 45 dealing with anabolic resistance, or women returning from injury or extended inactivity. For most recreational women training 3–4 days per week, 1.6–1.8g/kg produces excellent results.
What a 30g Leucine-Threshold Meal Looks Like (With Food Examples)
The leucine threshold (~2.5–3g leucine per meal) is consistently reached when you consume approximately 30g of high-quality protein — particularly from animal sources, which tend to have 7–11% leucine content by weight.
Foods that deliver approximately 30g of protein (and enough leucine to hit the threshold):
| Food | Serving Size | Protein | Notes |
|---|---|---|---|
| Chicken breast (cooked) | ~110g (4 oz) | ~30g | Complete amino acid profile |
| Salmon (cooked) | ~130g (4.5 oz) | ~30g | Plus omega-3s |
| Greek yogurt (0% fat) | ~400g (1.5 cups) | ~28–30g | Easy, no-cook option |
| Eggs (whole) | 5 large eggs | ~30g | May combine 3 eggs + whites |
| Cottage cheese | ~300g (1.25 cups) | ~30g | High leucine content |
| Whey protein powder | ~35g (1 large scoop) | ~28–30g | Fast-absorbing, ideal post-workout |
| Edamame (cooked) | ~400g (2.5 cups) | ~30g | Plant-based complete protein |
| Tempeh | ~170g (6 oz) | ~30g | Fermented soy, high bioavailability |
For plant-based women: Plant proteins typically contain 6–8% leucine (vs. 8–11% in animal proteins), meaning you may need to consume slightly more total protein — approximately 35g — to reach the same leucine threshold. Combining leucine-rich plants (edamame, soy, pea protein) improves this ratio.
Post-Workout Timing: Is the ‘Anabolic Window’ Real?
The “anabolic window” — the idea that you must eat protein within 30 minutes after exercise or lose all your gains — is largely a myth for most women. Current research suggests the muscle protein synthesis response to exercise remains elevated for up to 24 hours after a session.
However, “largely a myth” doesn’t mean timing is irrelevant. The ISSN recommends spacing protein intake every 3–4 hours to maximize the anabolic response. If you train fasted (without eating), the “window” becomes more important because your body is in a negative protein balance. In that case, consuming 20–30g of high-quality protein immediately after training helps switch your body from breakdown (catabolism) to building (anabolism).
- Practical Timing Rules:
- Total Daily Intake Wins: Consistently hitting your g/kg target matters far more than exact timing.
- Pre-Sleep Protein: Consuming 30–40g of a slow-digesting protein (like cottage cheese or casein powder) before bed supports overnight muscle repair, particularly relevant for women over 40.
- Training Fasted? Eat immediately after. Training Fed? You have a flexible 2–3 hour window.
Maintenance vs. Growth: Understanding the Energy Balance
You cannot build significant muscle tissue out of thin air. While “body recomposition” (losing fat and gaining muscle simultaneously) is possible, especially for beginners or those returning to training, optimizing for growth usually requires a slight energy surplus alongside high protein.
- Maintenance: Eating at calorie maintenance with high protein (1.6g/kg) helps you keep current muscle while slowly improving tissue quality.
- Growth: Eating a small surplus (~200-300 calories) with high protein (1.8-2.2g/kg) provides the raw materials and energy needed to build new muscle tissue efficiently.
Many women stall because they try to build muscle while in a calorie deficit. If your goal is significant hypertrophy, fuel the work.
Your Muscle-Building Protein Calculator
Use this simple reference to determine your muscle-building target:
Step 1: Find your weight in kilograms (lbs ÷ 2.2). Step 2: Choose your multiplier based on training frequency.
| Training Frequency | Multiplier | 68kg Example | 75kg Example |
|---|---|---|---|
| 2–3 days/week (moderate) | 1.6g/kg | 109g/day | 120g/day |
| 4–5 days/week (active) | 1.8g/kg | 122g/day | 135g/day |
| 5–6 days/week (high volume) | 2.0–2.2g/kg | 136–150g/day | 150–165g/day |
| 40+ with anabolic resistance | 2.0g/kg minimum | 136g/day | 150g/day |
Step 3: Divide across 3–4 meals, with each meal containing at least 30g.
Step 4 — Increase Your Protein Intake After 40

After 40, the rules of protein change significantly — and most women are never told this. Your body processes protein less efficiently, hormonal shifts accelerate muscle loss, and bone density becomes increasingly dependent on adequate protein intake. Our review of the research on aging and muscle shows this clearly: the same woman who thrived on 90g of protein at 35 may need 130g at 55 to maintain the same muscle mass. For specific exercises to pair with this intake, see our guide on strength training for combatting age-related muscle loss.
What Is Anabolic Resistance and Why It Hits After 40
Anabolic resistance is the reduced ability of aging muscle to respond to protein and exercise. In practical terms, a 55-year-old woman needs more protein per meal than a 30-year-old woman to trigger the same muscle-building signal — not because her muscles don’t work, but because the cellular sensitivity to leucine decreases with age.
Research confirms that older adults displaying anabolic resistance require approximately 40g of high-quality protein per meal — not 25–30g — to maximally stimulate muscle protein synthesis. Studies in PubMed have shown that older adults often need at least 1.17g/kg just to maintain function, with optimal intakes closer to 1.5g/kg.
This is why the standard “eat 20g of protein per meal” advice, still repeated by many generic health websites, is genuinely inadequate for women over 40. The threshold rises just as the body becomes more important to protect.
Your Protein Target by Decade: 40s, 50s, 60s, and 70s+
Each decade past 40 carries specific physiological changes that affect how much protein you need. Here is the evidence-based breakdown:
| Decade | Key Change | Protein Target | Priority Focus |
|---|---|---|---|
| 40s | Declining estrogen begins; early sarcopenia risk | 1.4–1.6g/kg | Build the habit before loss accelerates |
| 50s (perimenopause) | Significant estrogen drop; muscle loss accelerates ~0.6%/year | 1.6–2.0g/kg | Counter hormonal muscle-wasting |
| 60s | Anabolic resistance pronounced; bone density critical | 1.8–2.0g/kg | Combine with resistance training + calcium |
| 70s+ | Appetite often reduced; risk of both undernutrition and falls | 1.8–2.2g/kg | Prioritize protein-dense foods; consider supplementation |
- Worked example: A 68kg woman across decades
- Age 40: 1.4g/kg = 95g/day
- Age 52: 1.8g/kg = 122g/day
- Age 62: 2.0g/kg = 136g/day
- Age 72: 2.0g/kg = 136g/day (minimum)
Stanford Lifestyle Medicine (2024) specifically recommends a floor of 1.2–1.6g/kg for adults over 50 simply to maintain current muscle mass — not to build it. Building requires the higher end or above.
The Menopause Protein Protocol: Why You Need 1.6–2.0g/kg
During perimenopause and menopause, estrogen loss directly impairs muscle protein synthesis — the cellular repair process that keeps your muscles strong and metabolically active. Research suggests postmenopausal women lose approximately 0.6% of muscle mass per year when protein intake is inadequate (Women’s Health Magazine, 2026). This loss may seem small, but over a decade it translates to 6% of total muscle — enough to meaningfully affect strength, metabolism, energy, and mobility.
The Menopause Protein Protocol within the Thriving Threshold Framework recommends:
- Target 1.6–2.0g/kg daily — starting in perimenopause, before significant muscle loss occurs.
- Distribute across 3–4 meals with a minimum of 30–40g per meal (due to anabolic resistance).
- Prioritize leucine-rich sources at each meal: eggs, Greek yogurt, cottage cheese, chicken, fish.
- Add resistance training at least 2–3 days per week — protein alone cannot fully compensate for the hormonal deficit; exercise amplifies the protein signal.
- Consider a pre-sleep protein snack (30g cottage cheese or casein protein) to support the overnight muscle repair cycle.
Individual needs vary. Consult a registered dietitian or your doctor before significantly changing your protein intake.
Protein and Bone Density: The Connection Competitors Miss
Adequate protein intake is critical for bone density — a connection that most women’s health content overlooks entirely. Bone is approximately 50% protein by volume. The matrix (scaffold) of bone is made of collagen protein; calcium and other minerals are deposited into that matrix. Without adequate dietary protein, the bone matrix weakens regardless of calcium intake.
This condition — the simultaneous loss of muscle and bone — is called osteosarcopenia, and it is estimated to affect a significant proportion of women over 65. Research suggests that women eating above the RDA for protein have better bone mineral density measures than those eating at or below 0.8g/kg. The combination of adequate protein + calcium + vitamin D + resistance exercise represents the most evidence-based strategy for bone preservation available to women over 40.
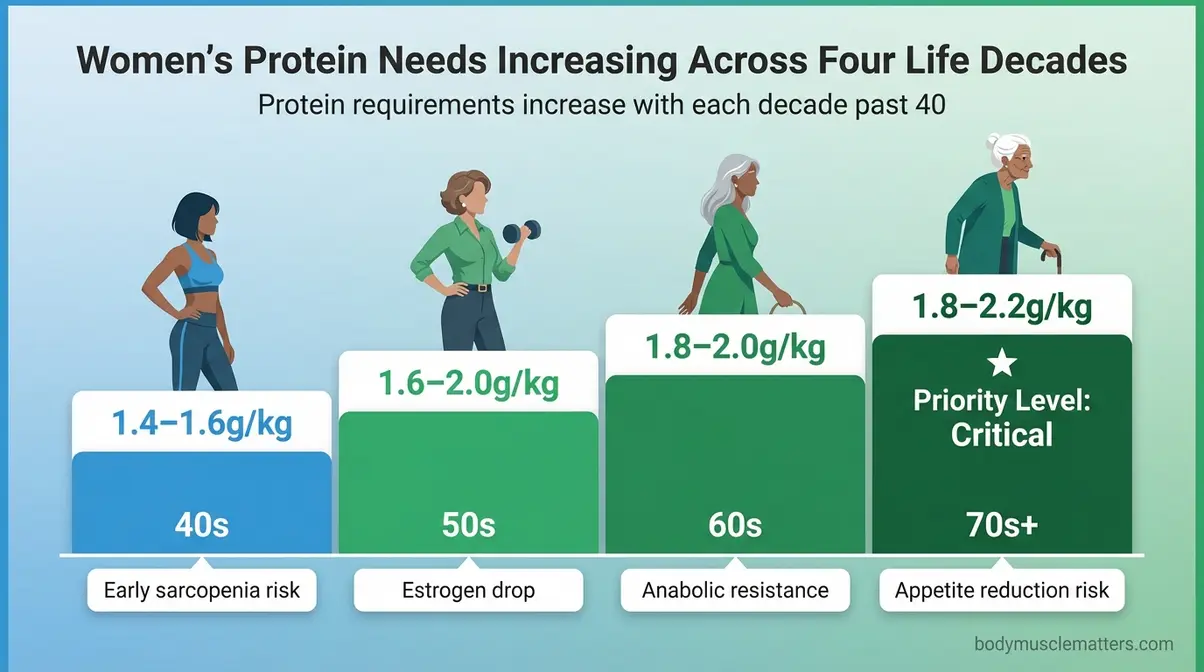
Caption: Protein requirements increase with each decade past 40 — the Thriving Threshold adjusts for both anabolic resistance and hormonal changes.
Step 5 — Adjust Your Protein Intake During Pregnancy and Breastfeeding
Protein needs shift significantly during pregnancy and breastfeeding. This section applies evidence-based guidance from ACOG (American College of Obstetricians and Gynecologists) and UCSF Health to help you meet your baby’s needs while protecting your own muscle mass.
This section contains medical guidance. Always consult your OB-GYN or registered dietitian for personalized prenatal nutrition advice.
Protein Needs by Trimester: A Week-by-Week Overview
Pregnancy dramatically increases your protein requirements, particularly from the second trimester onward, when fetal tissue growth accelerates. The American Pregnancy Association recommends 75–100g of protein per day during pregnancy, representing a significant increase from the pre-pregnancy baseline of ~46g/day for sedentary women.
Here is a practical trimester breakdown:
| Trimester | Weeks | Key Development | Protein Target |
|---|---|---|---|
| First Trimester | 1–12 | Organ formation begins; nausea may limit intake | 60–75g/day (baseline + ~14g increase) |
| Second Trimester | 13–26 | Rapid fetal growth; muscle and organ development | 75–100g/day |
| Third Trimester | 27–40 | Brain development; fetal weight gain peaks | 80–110g/day |
Practical note on first trimester nausea: If morning sickness limits your ability to eat large protein portions, focus on frequent small protein-rich snacks — Greek yogurt, hard-boiled eggs, nut butter on crackers — rather than full meals. Even 15–20g of protein in a small snack advances your daily total. PubMed research emphasizes that adequate protein during this period is crucial for preventing low birth weight.
Individual needs vary. Consult a registered dietitian or your doctor before significantly changing your protein intake during pregnancy.
Breastfeeding and Protein: How Much More Do You Need?
Breastfeeding increases your protein needs by approximately 25 grams per day above your pre-pregnancy baseline. According to international dietary guidelines, exclusively breastfeeding women need an additional 19g/day in the first six months and an additional 13g/day after six months as complementary foods are introduced (European Food Safety Authority data, as compiled in nutrition guidance).
- In practice, this means:
- Breastfeeding target: Your normal baseline + 25g/day
- For a 68kg active woman: 95g (baseline) + 25g = ~120g/day
- Spread across 4–5 smaller meals or snacks to manage the increased demand
Protein supports milk production quality and helps your body recover from childbirth — particularly important for rebuilding the lean muscle mass that may have been lost during pregnancy.
Safe Protein Sources During Pregnancy (Including Mercury-Safe Fish)
Choosing protein sources wisely during pregnancy protects both your nutritional needs and your baby’s development. The following guide incorporates ACOG’s fish safety recommendations:
Safest protein sources during pregnancy:
| Source | Protein | Safety Note |
|---|---|---|
| Eggs (fully cooked) | ~6g per egg | Safe; avoid raw/undercooked |
| Greek yogurt (pasteurized) | ~18–20g per cup | Safe; choose pasteurized |
| Chicken (fully cooked) | ~30g per 110g serving | Safe; cook to 165°F |
| Salmon (wild-caught) | ~30g per 130g serving | 2–3 servings/week; low mercury |
| Sardines (canned in water) | ~22g per 100g | Excellent choice; very low mercury |
| Lentils and legumes | ~18g per cup cooked | Plant-based; combine with other sources |
| Cottage cheese (pasteurized) | ~14g per ½ cup | Safe; choose pasteurized |
| Shrimp | ~20g per 100g | Low mercury; safe 2–3 servings/week |
Fish to avoid during pregnancy (high mercury risk per ACOG): shark, swordfish, king mackerel, tilefish, bigeye tuna. Limit albacore (white) canned tuna to 6 oz/week.
Step 6 — Choose Your Protein Sources and Build a Meal Plan

Knowing your target is step one. Hitting it consistently requires knowing which foods to lean on and how to build meals that reach 30g per sitting without turning every meal into a production. This step makes the numbers practical. For specific ideas on how to structure your plate, check out our guide to creating a balanced high-protein plate.
Top 10 High-Protein Foods for Women (Animal and Plant-Based)
Building your diet around these 10 foods makes it realistic to hit your daily protein target whether you eat meat, prefer plants, or eat a combination of both.
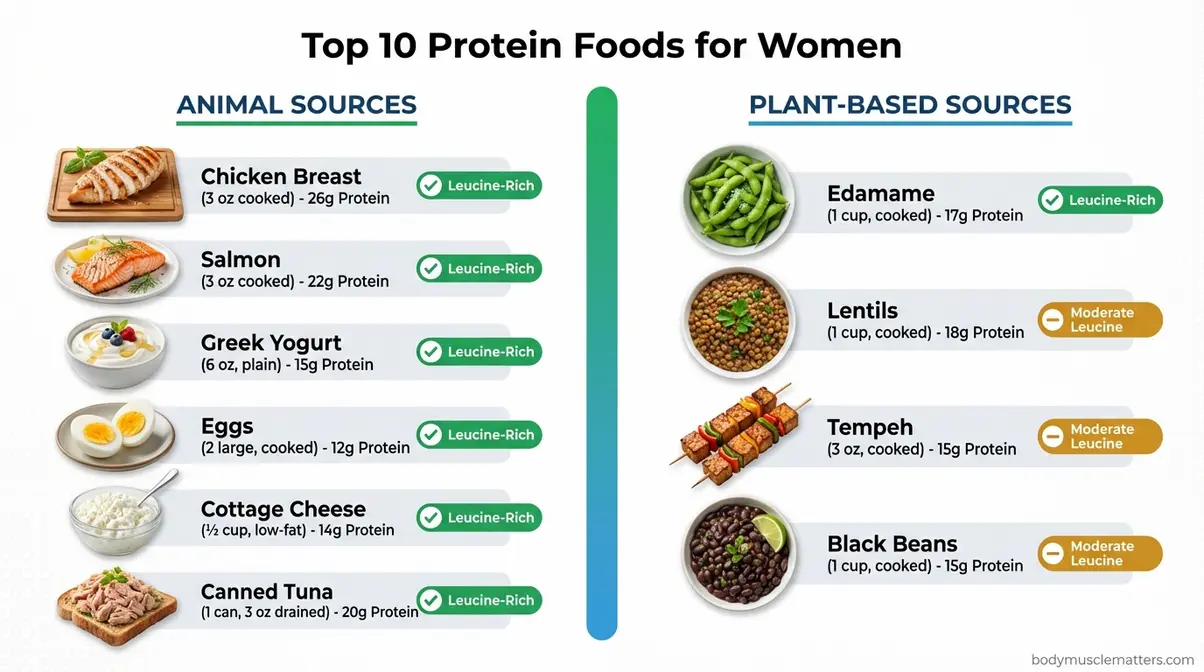
Caption: Combining animal and plant protein sources gives you the full amino acid spectrum while varying flavor, cost, and preparation.
| Food | Serving | Protein | Type | Leucine-Rich? |
|---|---|---|---|---|
| Chicken breast (cooked) | 110g (4 oz) | ~30g | Animal | ✅ Yes |
| Salmon | 130g (4.5 oz) | ~30g | Animal | ✅ Yes |
| Greek yogurt (0% fat) | 1 cup (245g) | ~18–22g | Animal | ✅ Yes |
| Eggs | 2 large | ~12g | Animal | ✅ Yes |
| Cottage cheese | ½ cup (113g) | ~14g | Animal | ✅ Yes |
| Canned tuna (in water) | 100g | ~22g | Animal | ✅ Yes |
| Edamame (cooked) | 1 cup (155g) | ~17g | Plant | ✅ Yes (soy) |
| Lentils (cooked) | 1 cup (200g) | ~18g | Plant | Moderate |
| Tempeh | 100g | ~19g | Plant | ✅ Yes (soy) |
| Black beans (cooked) | 1 cup (172g) | ~15g | Plant | Moderate |
For plant-based women: Focus on soy-based proteins (edamame, tempeh, tofu) as your primary protein anchor, since soy is a complete protein with a higher leucine content than most legumes. Combine rice with beans, or pair lentils with quinoa, to ensure you’re getting all essential amino acids across the day.
Your Protein Intake Reference Chart (g/kg by Body Weight and Goal)
This chart is your at-a-glance reference. Print it, screenshot it, or bookmark this page.
| Body Weight | Sedentary (1.0g/kg) | Weight Loss (1.4g/kg) | Active (1.6g/kg) | Muscle Building (2.0g/kg) |
|---|---|---|---|---|
| 50 kg (110 lbs) | 50g | 70g | 80g | 100g |
| 60 kg (132 lbs) | 60g | 84g | 96g | 120g |
| 68 kg (150 lbs) | 68g | 95g | 109g | 136g |
| 75 kg (165 lbs) | 75g | 105g | 120g | 150g |
| 82 kg (180 lbs) | 82g | 115g | 131g | 164g |
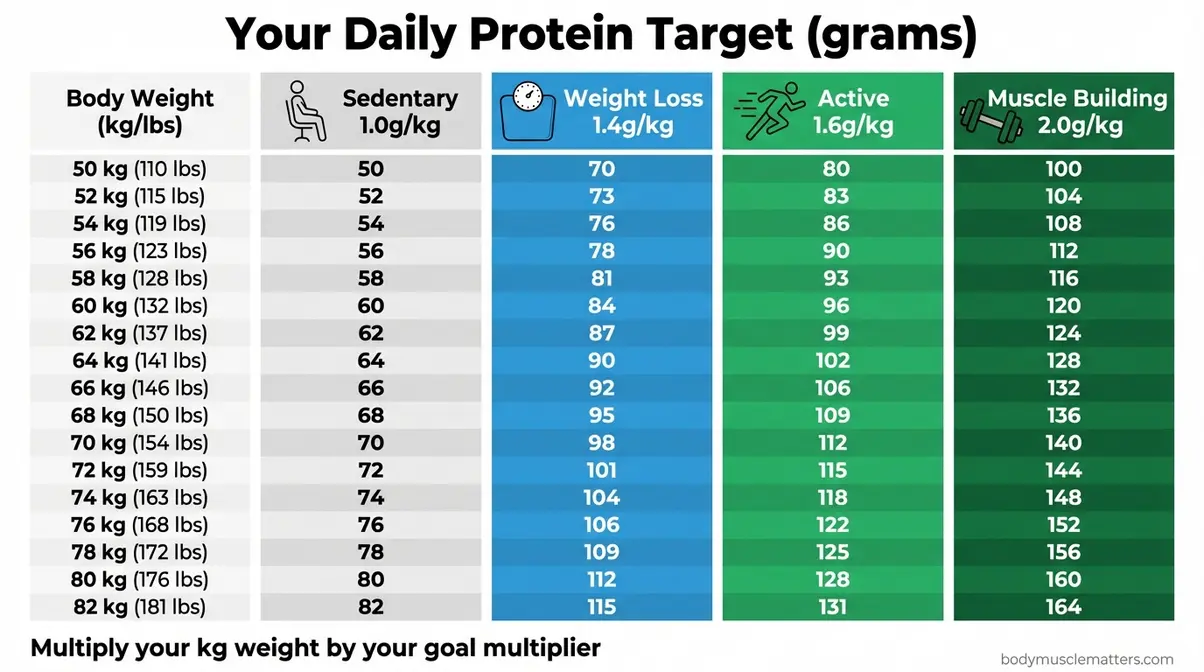
Caption: Cross-reference your body weight with your current goal to find your personal Thriving Threshold.
Practical Tips to Hit Your Daily Target Without Obsessing
Many women find tracking protein liberating at first — and exhausting within two weeks. These strategies let you hit your target without turning every meal into a spreadsheet exercise:
- Anchor every meal with protein first. Before choosing your carbohydrate or fat component, decide on the protein. Ask: “What’s the 30g protein base for this meal?”
- Stock your refrigerator with ready-to-eat protein. Pre-cooked chicken, hard-boiled eggs, and Greek yogurt remove the prep barrier for busy days.
- Use the “palm rule” as a rough estimate. One palm-sized serving of meat or fish = approximately 25–30g of protein. Two large eggs = ~12g. One cup of Greek yogurt = ~18–22g.
- Additional Tips:
- Add protein to meals you already love. Stir Greek yogurt into sauces, add cottage cheese to pasta, blend a scoop of protein powder into oatmeal.
- Track for two weeks, then internalize. Two weeks of tracking gives most women enough pattern recognition to estimate accurately without weighing food daily.
Individual needs vary. Consult a registered dietitian or your doctor before significantly changing your protein intake.
Troubleshooting — Is High Protein Intake Safe? Kidney Health and Upper Limits
This section directly addresses the kidney safety concern that stops many women from increasing their protein intake. Understanding the actual evidence — rather than common myths — empowers you to make an informed decision. For more detailed safety guidelines, review our article on safe upper limits for protein intake.
The Kidney Damage Myth: What the Research Actually Shows
For healthy women with normal kidney function, research does not support a link between high-protein diets (up to 2.0g/kg) and kidney damage. This is the most important nuance: the kidney concern applies to women who already have kidney disease, not to the general population.
A 2024 meta-analysis published in PubMed found that higher dietary protein intake — particularly from plant and fish sources — was actually associated with a lower risk of chronic kidney disease in the general population (PubMed, 2024). This aligns with Mayo Clinic’s explanation that high-protein diets may stress kidneys that are already compromised, but do not cause damage in healthy kidneys.
The concern about kidney damage from protein originated largely from studies of people who already had kidney disease, where high protein intake can accelerate existing damage. Applying this finding to healthy women was a scientific overstep that became medical folklore. Research from 2024 suggests the picture is nuanced and that source of protein matters: plant and fish proteins appear to have a more favorable profile than very high animal protein intake.
The practical summary: Eating 1.2–2.0g/kg of protein per day is not a kidney risk for healthy women without pre-existing kidney conditions. If you have any kidney concerns, see the next section.
Warning Signs You’re Eating Too Much Protein
Overconsumption of protein — typically above 2.5–3g/kg per day for extended periods — may produce recognizable symptoms. Most women eating 1.2–2.0g/kg will not experience these. They are more relevant for women who are significantly over-shooting targets, often via supplements.
- Signs that your intake may be too high:
- Persistent bad breath (ammonia-like smell — from excess nitrogen processing)
- Increased thirst and more frequent urination
- Digestive discomfort: bloating, constipation, or diarrhea (particularly with high supplement use)
- Fatigue or nausea (particularly with very rapid intake increases)
- Unexplained weight gain (protein still contributes to calorie surplus if total calories exceed needs)
These symptoms typically resolve by reducing intake to the recommended 1.2–2.0g/kg range and ensuring adequate hydration. Very high protein intake without sufficient water intake puts unnecessary strain on the kidneys’ filtering capacity — not because protein damages healthy kidneys, but because hydration is needed to excrete the byproducts of protein metabolism.
When to Limit Protein: CKD, One Kidney, and Medical Conditions
⚠️ Important medical guidance: if you have any of the following conditions, the general recommendations in this article do NOT apply to you. Speak with your nephrologist or registered dietitian before changing your protein intake.
Conditions requiring protein restriction or individualized guidance:
| Condition | General Guidance | Why |
|---|---|---|
| Chronic Kidney Disease (CKD) Stages 3–5 | Low-protein diet (~0.6–0.8g/kg) recommended | High protein accelerates kidney function decline in CKD |
| One kidney (functional) | Moderate protein; often ≤1.0g/kg | Single kidney handles full filtration load; excess protein increases workload |
| Dialysis patients | Higher protein (1.2–1.4g/kg) often recommended | Dialysis removes protein; needs are paradoxically higher |
| Lupus nephritis or PKD | Individualized; usually restricted | Inflammatory kidney conditions worsen with high protein load |
| Liver disease (cirrhosis) | Individualized; requires medical supervision | Impaired protein metabolism |
The National Kidney Foundation recommends that people with CKD limit protein and favor plant-based proteins, which produce fewer nitrogen byproducts. If you have been diagnosed with kidney disease at any stage, your renal diet protein target must be set by a registered dietitian or nephrologist — not by a general guide like this one.
Individual needs vary. Consult a registered dietitian or your doctor before significantly changing your protein intake, especially if you have kidney disease or a chronic health condition.
Common Mistakes That Undermine Your Protein Goals
Even women who understand the framework consistently undermine their progress with a handful of predictable patterns. Recognizing these mistakes before you make them saves weeks of frustration.
The Three Most Common Protein Distribution Mistakes
Mistake 1: Back-loading protein at dinner The most common pattern among women is eating 15–20g of protein at breakfast and lunch, then trying to eat 50–60g at dinner to “catch up.” This approach fails the leucine threshold test at breakfast and lunch — two out of three meals produce minimal muscle repair signal. Result: even if total daily protein looks adequate on paper, the physiological benefit is roughly half of what it would be from even distribution.
Fix: Plan breakfast first. Make 30g of protein your breakfast non-negotiable. Everything else is easier once the morning meal is structured.
Mistake 2: Confusing low-calorie foods with high-protein foods Many foods marketed as “healthy” or “light” are very low in protein. A large green salad with vegetables and vinaigrette may have 3–5g of protein. A rice cake with hummus has approximately 4–6g. Almond milk has 1g per cup, compared to cow’s milk at 8g. Treating these foods as “protein sources” creates a significant gap between perceived intake and actual intake.
Fix: Learn the protein content of your 10–15 most frequently eaten foods. Anything under 15g per serving is a protein supplement, not a protein anchor.
Mistake 3: Relying on protein bars or shakes as the primary source Many protein bars marketed to women contain 10–15g of protein alongside 20–30g of sugar and highly processed ingredients. While protein powders and shakes are convenient tools, building your primary protein intake around supplements — rather than whole foods — means missing the additional nutritional benefits (vitamins, minerals, fiber, healthy fats) that whole protein sources provide.
Fix: Use supplements to fill gaps (a post-workout shake, a pre-sleep protein snack), not as meal replacements. Whole food sources should represent at least 70–80% of your daily protein intake.
When to Work With a Registered Dietitian
A registered dietitian (RD) is the right partner when:
- You have a medical condition — kidney disease, liver disease, diabetes, eating disorder history, or YMYL-level complexity in your health picture. General guides cannot safely advise you.
- You are pregnant or breastfeeding and want individualized prenatal nutrition beyond general guidance.
- You are on GLP-1 medications and struggling to hit protein targets despite appetite suppression.
- The numbers feel overwhelming — an RD can create a personalized meal plan that hits your targets without requiring you to track every meal forever.
- You’ve been consistently under-eating protein for years and want to ensure a gradual, safe increase.
- You’re postmenopausal and experiencing rapid muscle loss — an RD combined with a physical therapist offers the most evidence-based combination for osteosarcopenia prevention.
Seek an RD who specializes in women’s health, sports nutrition, or aging — not a generalist. Look for the credential “RD” (Registered Dietitian) or “RDN” (Registered Dietitian Nutritionist) — these are regulated, evidence-based credentials.
Frequently Asked Questions
Is 100g of protein too much for a woman?
For most women, 100g of protein per day is not too much — it’s close to the optimal range. A 68kg (150lb) active woman targeting 1.4–1.6g/kg needs 95–109g daily, making 100g a completely appropriate target. Research consistently supports intakes of 1.2–2.0g/kg without adverse effects in healthy women (UCLA Health, 2025; Stanford Lifestyle Medicine, 2024). The concern about “too much” protein applies primarily to women with diagnosed kidney disease, not the general population. If you feel any digestive discomfort when increasing protein quickly, increase gradually over 2–3 weeks and drink adequate water throughout the day.
How much protein should I eat in a day as a female?
The evidence-based answer for most women is 1.2–2.0g of protein per kilogram of body weight per day, depending on your goal and life stage. For a 150lb (68kg) woman, that means roughly 82–136g/day. The government’s 0.8g/kg RDA (54g/day for a 68kg woman) is a survival minimum, not an optimal health target. Use the Thriving Threshold Framework in Step 1 to calculate your personal number: multiply your weight in kg by your goal multiplier (1.4 for weight loss, 1.6 for active maintenance, 2.0 for muscle building or menopause). Consult a registered dietitian for personalized guidance.
Is 70 grams of protein enough for a woman?
For a smaller, sedentary woman, 70g may be adequate. For most active women or women over 40, 70g is likely insufficient. A 55kg (121lb) woman targeting 1.2–1.4g/kg needs 66–77g/day — so 70g sits at the low end of her range. A 68kg (150lb) woman at the same multiplier needs 82–95g. Women over 40 dealing with anabolic resistance and perimenopause need 1.6–2.0g/kg, meaning a 68kg woman needs 109–136g daily to maintain muscle mass effectively. If your current intake is 70g and you are over 40 or actively training, this is likely the variable limiting your results.
How much protein should someone with one kidney eat?
Women with one functioning kidney should NOT follow the general recommendations in this guide without medical supervision. A single kidney performs the full filtration workload of two kidneys, meaning excess protein metabolism increases its functional burden over time. The National Kidney Foundation recommends that people with a single kidney work with a nephrologist or registered dietitian to set an individualized protein target — generally moderate (often ≤1.0g/kg/day), with plant proteins preferred over animal proteins where possible. Regular kidney function monitoring (eGFR and creatinine tests) is essential when adjusting protein intake with one kidney.
How much protein to lose weight as a woman?
For weight loss, research supports 1.2–1.6g of protein per kilogram of body weight per day — significantly higher than the standard RDA. This range preserves lean muscle mass during a calorie deficit (preventing metabolic slowdown), increases the thermic effect of food (burning more calories through digestion), and dramatically improves satiety (reducing hunger between meals). For a 68kg (150lb) woman, that means 82–109g/day. Start at 1.2g/kg (82g/day) and increase toward 1.6g/kg as you add resistance training. Distribute protein across 3–4 meals with at least 30g per sitting for maximum muscle-preserving benefit. Consult a registered dietitian for personalized guidance.
Conclusion
For health-conscious women at every life stage, protein intake is the single most under-optimized nutritional variable affecting energy, body composition, and long-term health. The government’s 0.8g/kg RDA — 54g/day for a 150lb woman — was designed to prevent deficiency, not to support active muscles, hormonal balance, or the physiological demands of perimenopause. Current evidence from Stanford Lifestyle Medicine (2024), UCLA Health (2025), and ISSN-aligned research consistently supports 1.2–2.0g/kg as the functional optimal range for most women, with higher targets for those over 45 or in muscle-building phases.
The Thriving Threshold Framework presented in this guide gives you more than a number — it gives you a system. Calculate your target using the g/kg formula. Structure each meal around the 30g leucine threshold. Adjust for your life stage: 1.4g/kg in your active 30s, 1.6–1.8g/kg in perimenopause, 2.0g/kg in postmenopause. These adjustments are not optional extras — they are the difference between maintaining your muscle, metabolism, and bone density through menopause and beyond, or losing them quietly while eating “healthy.”
Your starting point is simple: pick up your bodyweight in kilograms, multiply by 1.4, and make that your protein target for the next 30 days. Restructure breakfast first — a 30g protein anchor in the morning changes the entire trajectory of your day. Track for two weeks to build pattern recognition, then trust your knowledge. If you are pregnant, have kidney disease, or are on GLP-1 medications, partner with a registered dietitian who specializes in women’s health — the investment pays for itself in avoided muscle loss and better metabolic outcomes for years ahead.
