
“Been weight training consistently for 3 years, 3–5 times a week but approaching 38 I’m hardly seeing any muscle gains.”
Sound familiar? If you’ve been hitting the gym consistently but wondering at what age do muscles stop growing — and whether that invisible cutoff has already passed — you’re not alone. This is one of the most common frustrations among dedicated, problem-aware adults in their 30s, 40s, and 50s.
Here’s the honest truth: without targeted resistance training, adults can lose 3% to 5% of their muscle mass every decade after age 30 (American College of Sports Medicine). That’s not a small number when you’re already continuously hitting the gym and barely seeing results. But the good news — and there’s a lot of it — is that this decline is neither inevitable nor irreversible.
In this guide, you’ll learn exactly when and why muscle growth slows, what science actually says about building muscle in your 30s, 50s, and even 70s, and the specific strategies that work at every age. You’ll walk away with a clear, decade-by-decade action plan you can start this week.
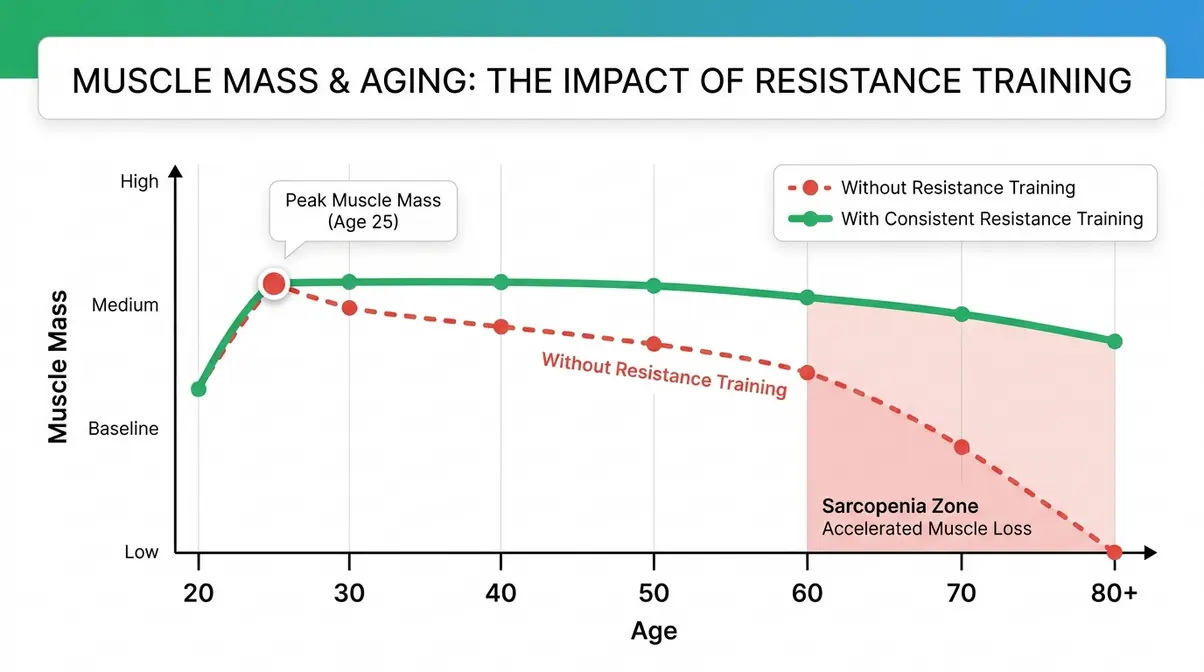
If you are wondering at what age do muscles stop growing, the answer is that they never truly stop. However, without resistance training, adults lose 3–5% of muscle mass per decade after 30 (ACSM). The Muscle Longevity Spectrum shows that every decade offers a viable growth window.
- After 30: Muscle mass peaks, then begins a slow, manageable decline
- After 60: Decline accelerates (sarcopenia), but resistance training reverses it
- At any age: Consistent training + 1.6–2.2g of protein per kg bodyweight = continued gains
- The Muscle Longevity Spectrum: Your training age matters more than your calendar age
The Muscle Aging Timeline: When Decline Begins
Muscle decline doesn’t happen overnight, and it certainly doesn’t happen the morning you turn 30. The process is gradual — almost imperceptibly slow in your 30s — then it picks up speed in your 60s if left unchecked. Understanding this timeline is the first step toward working with your biology rather than against it.
Peak Muscle Mass: Your 20s and 30s
Most people reach their peak muscle mass somewhere between ages 20 and 30. After that, a slow, quiet process of change begins. Research published in the Journal of Cachexia, Sarcopenia and Muscle confirms that muscle fiber size and number begin declining gradually from the late 20s onward, which is key to understanding muscle growth across different ages. The process becomes measurable in your mid-30s (Janssen et al., PMC, 2000).
For the person approaching 38 and seeing fewer gains, this is the biology behind that frustration. Your body is no longer in the “easy build” phase of early adulthood. Anabolic hormones — the chemical messengers that tell your muscles to grow — are beginning their long, slow decline. But here’s what matters: “declining” does not mean “gone.” You can absolutely still gain muscle after 30. The rules just change slightly.
Why this matters: if you understand that your 30s represent the start of a slow transition — not a cliff edge — you can adapt your training and nutrition ahead of the curve rather than chasing lost ground.
Muscle Loss in Your 40s and 50s
The 40s and 50s are where the shift becomes more noticeable. Research suggests adults lose roughly 1% to 2% of muscle mass per year starting in their 40s if they don’t actively counteract it (Harvard Health Publishing). That cumulative loss adds up: by your mid-50s, you may have lost 10–15% of the muscle you had at 30 without realizing it.
Protein’s role becomes critically important in this decade. Older muscle tissue is less efficient at using dietary protein for repair and growth — a phenomenon called anabolic resistance (more on that shortly). This is why many people in their 50s feel like they’re working just as hard in the gym but recovering more slowly and seeing fewer results. They’re right. But the solution isn’t to give up — it’s to eat more protein and train smarter.
Accelerated Decline After Age 60
After age 60, muscle loss can accelerate to 1.5% to 2% per year, a condition clinicians call sarcopenia (the medical term for age-related muscle loss that impairs physical function). According to the National Institute on Aging, sarcopenia affects an estimated 10–30% of adults over 60, and the prevalence rises steeply with each passing decade (NIA).
The encouraging finding from clinical research is this: even at 70 or 80 years old, muscles retain the biological machinery to grow. The stimulus just needs to be consistent and adequately challenging. Physical therapists who work with older adults routinely report that patients who begin resistance training in their 60s and 70s see measurable strength and muscle gains within 8–12 weeks — timelines comparable to younger beginners.
This shift toward accelerated decline after 60 creates the conditions for why the 70s training protocol (covered later) must look different from a 30-year-old’s program — not easier, necessarily, but smarter.
What Age Is Hardest to Gain Muscle?
Most people find muscle building progressively harder starting in their 40s and 50s, when anabolic resistance — the reduced sensitivity of muscle tissue to growth signals — becomes measurable. This doesn’t mean it’s impossible; it means the required stimulus (training intensity, protein intake) needs to be higher. Research consistently shows that adults in their 40s and 50s can still achieve meaningful hypertrophy with appropriate programming and nutrition. The difficulty increases gradually, not suddenly, and smart training largely compensates for biological changes.
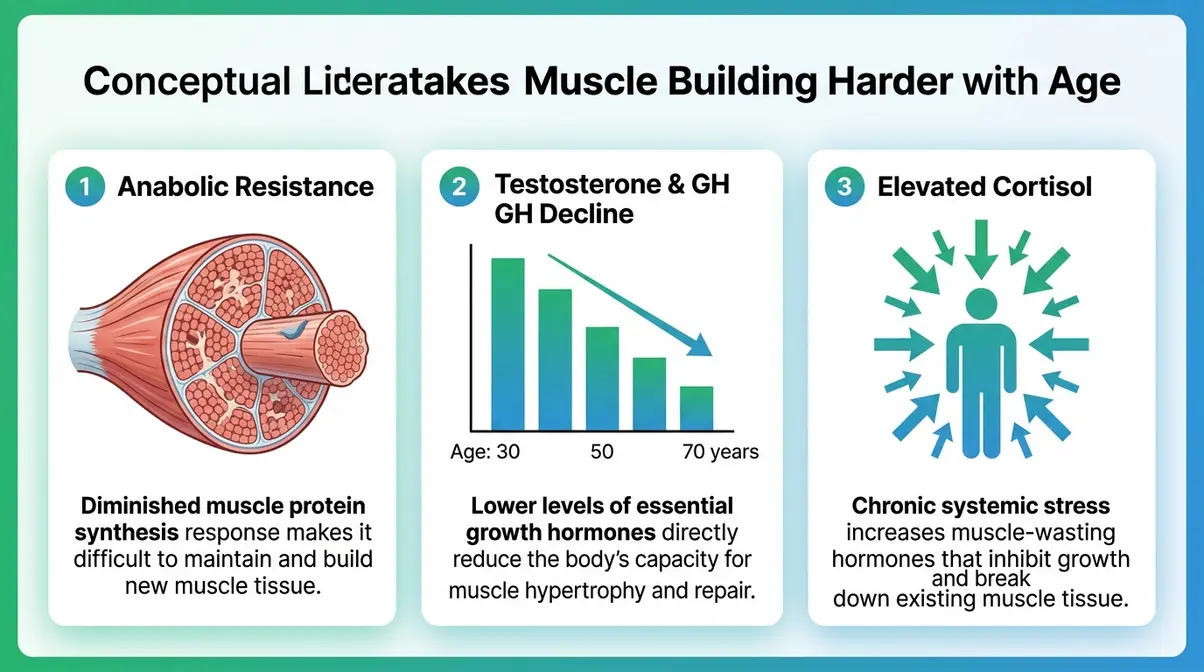
Why Building Muscle Gets Harder With Age
The biology behind age-related muscle loss is not a mystery. Several well-documented hormonal and cellular shifts work together to make muscle building progressively more challenging after your 30s. Knowing what these shifts are — and why they happen — helps you understand exactly which levers you can pull to fight back.
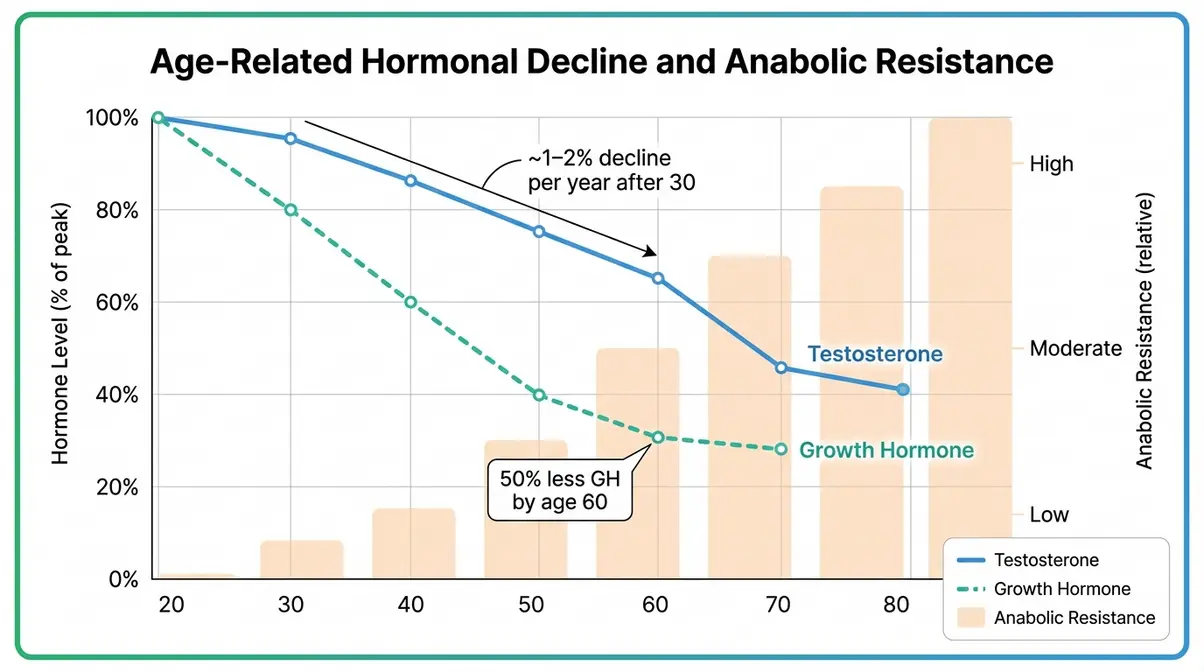
Testosterone and Growth Hormone
Testosterone is the primary anabolic (muscle-building) hormone in the body. It signals muscle fibers to repair and grow after training stress. After age 30, testosterone levels in men decline by approximately 1% to 2% per year (Hospital for Special Surgery, 2026). Women have far lower testosterone to begin with, but they also experience a meaningful drop, particularly around menopause.
Growth hormone (GH) works alongside testosterone to stimulate muscle protein synthesis (the process of building new muscle proteins). GH secretion decreases significantly with age — by age 60, many adults produce roughly 50% less growth hormone than they did at 20 (PMC, 2000). Together, these two declines create a less anabolic environment in your body, meaning the same workout that built muscle at 25 produces a smaller signal at 45.
Why this matters: you can partially compensate for lower hormone levels by increasing training volume, prioritizing compound movements, ensuring adequate sleep, and getting essential vitamins for muscle development — all of which naturally boost testosterone and GH within normal ranges.
Anabolic Resistance Explained
Anabolic resistance is the term researchers use to describe a reduced sensitivity of aging muscle to the signals that normally trigger growth. Think of it like this: if testosterone is a text message telling your muscles to grow, anabolic resistance means the phone’s signal has gotten weaker. The message is still being sent — it just doesn’t land as clearly.
Research published in PMC (Churchward-Venne et al., 2012) demonstrates that older muscle tissue requires a higher dose of protein — and a more forceful training stimulus — to achieve the same anabolic response as younger muscle. Specifically, studies suggest that older adults need to consume 0.4g of protein per meal (rather than the 0.25g threshold that works for younger adults) to maximally stimulate muscle protein synthesis.
This is a critical insight. It means the plateau you feel isn’t imaginary — it’s biologically real. But it’s also solvable with targeted adjustments to your protein intake and training intensity.
High Cortisol: The Hidden Muscle Killer
Cortisol is your body’s primary stress hormone. In short bursts, it’s helpful — it sharpens focus and mobilizes energy. But chronically elevated cortisol actively breaks down muscle tissue (a process called catabolism) and suppresses the anabolic hormones needed to rebuild it.
The five most recognizable signs of chronically high cortisol are: unexplained weight gain (especially around the midsection), persistent fatigue despite adequate sleep, increased muscle weakness, mood changes like irritability or anxiety, and slow recovery from workouts. If several of these sound familiar, cortisol may be undermining your training results.
Research from the Cleveland Clinic notes that chronic psychological stress — common in adults aged 35–55 managing careers, families, and financial pressures simultaneously — is one of the primary drivers of elevated cortisol. Evidence suggests that prioritizing 7–9 hours of sleep, limiting training sessions to under 60 minutes, and managing life stress directly improve cortisol regulation and, consequently, muscle retention. Can you build muscle with high cortisol? Yes — but you’re fighting an uphill battle. Lowering cortisol is as important as lifting weights.
GLP-1 Medications and Lean Muscle Loss
This is a topic competitors are almost entirely ignoring, and it matters enormously right now. GLP-1 receptor agonists — medications like semaglutide (sold as Ozempic and Wegovy) — have become widely prescribed for weight loss and type 2 diabetes management. They work by suppressing appetite and slowing gastric emptying, leading to significant caloric restriction and rapid weight loss.
The concern: a significant portion of the weight lost on GLP-1 medications is lean muscle mass, not just fat. Research cited by UCLA Health (2026) found that in some trials, up to 25–39% of total weight loss on semaglutide came from lean mass. For an older adult already contending with sarcopenia, this is a serious consideration.
Can you gain muscle on GLP-1? The answer, according to current evidence, is yes — but only with a deliberate, concurrent resistance training program and aggressive protein intake (targeting the upper range of 1.6–2.2g per kg of bodyweight). If you are currently on a GLP-1 medication, talk to your prescribing physician about incorporating structured resistance training before or alongside your medication course.
Bones vs. Muscles: When Growth Finishes
A common point of confusion is conflating skeletal growth with muscle growth. These are two entirely different biological processes with very different timelines — and understanding the difference is genuinely reassuring.
When Do Bones Stop Growing?
Your bones grow from specialized areas called growth plates (also called epiphyseal plates) — regions of cartilage near the ends of long bones that gradually harden into solid bone as you age. The closure of growth plates marks the end of height gain and structural skeletal growth.
For most people, growth plates fully close between ages 16 and 25, with girls typically finishing earlier (around 16–18) and boys somewhat later (around 18–21). This means that by your mid-20s, your hands, fingers, wrists, and long bones have reached their permanent skeletal dimensions. The bones themselves no longer lengthen — though bone density continues to change throughout life.
This is entirely separate from muscle. Bone growth is governed by growth hormone and genetic programming during adolescence. Muscle growth is governed by a different set of signals that remain active — and responsive — throughout your entire lifespan.
Why Muscle Growth Potential Continues
Here is the fundamental distinction that changes everything: muscle fibers do not have a closing date. Unlike bones, muscle tissue is continuously remodeled — broken down and rebuilt — in response to mechanical stress (exercise), nutritional input (protein), and hormonal signaling.
The biological mechanism behind this is the activation of satellite cells — specialized stem cells that sit alongside muscle fibers and are recruited whenever a muscle is damaged or stressed by training. Research shows that satellite cell activation occurs in response to resistance training in adults well into their 80s (Churchward-Venne et al., PMC, 2012). The activation is less efficient in older adults, but it still happens.
This is the scientific basis for The Muscle Longevity Spectrum: muscle growth potential exists on a continuous, lifelong spectrum. It is not switched off at 30, 40, or 70. The conditions required to trigger it simply become more specific with age — demanding more precise training, more protein, and more recovery time.
Evidence: Building Muscle at Any Age
The most powerful antidote to age-related fitness anxiety isn’t motivation — it’s data. Clinical research on muscle building in older adults has produced results that consistently surprise people. Let’s look at what the evidence actually shows.
Clinical Studies on 70-Year-Olds
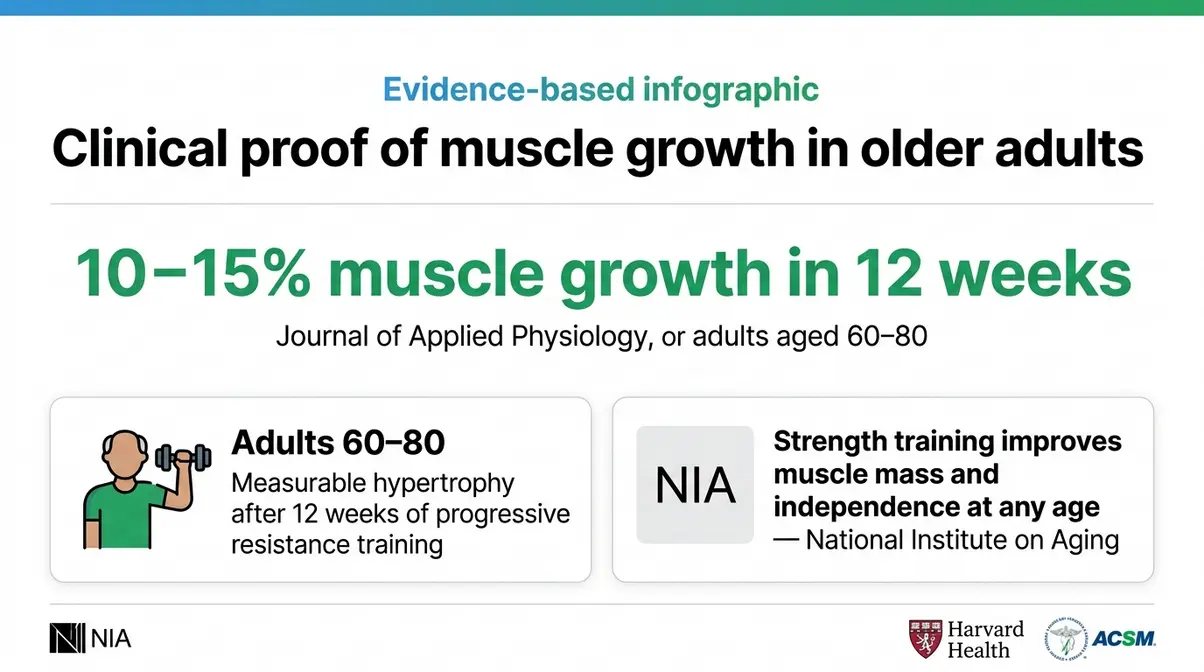
The landmark HERITAGE Family Study and subsequent resistance training trials have demonstrated something remarkable: older adults — including those in their 70s and 80s — show measurable hypertrophy (muscle fiber growth) in response to progressive resistance training. A widely cited study published in the Journal of Applied Physiology found that men and women aged 60–80 who performed resistance training three times per week for 12 weeks increased muscle cross-sectional area by 10–15%, comparable to gains seen in younger adults following the same program.
The National Institute on Aging summarizes the evidence clearly: “Strength training can help older adults maintain their independence, improve balance and coordination, reduce the risk of falls, and yes — increase muscle mass” (NIA).
The takeaway is direct: a 70-year-old who begins resistance training can absolutely still build muscle. The rate of gain may be slower than at 25, and the recovery window longer, but the biological pathway is open. Waiting is the only thing that closes it permanently.
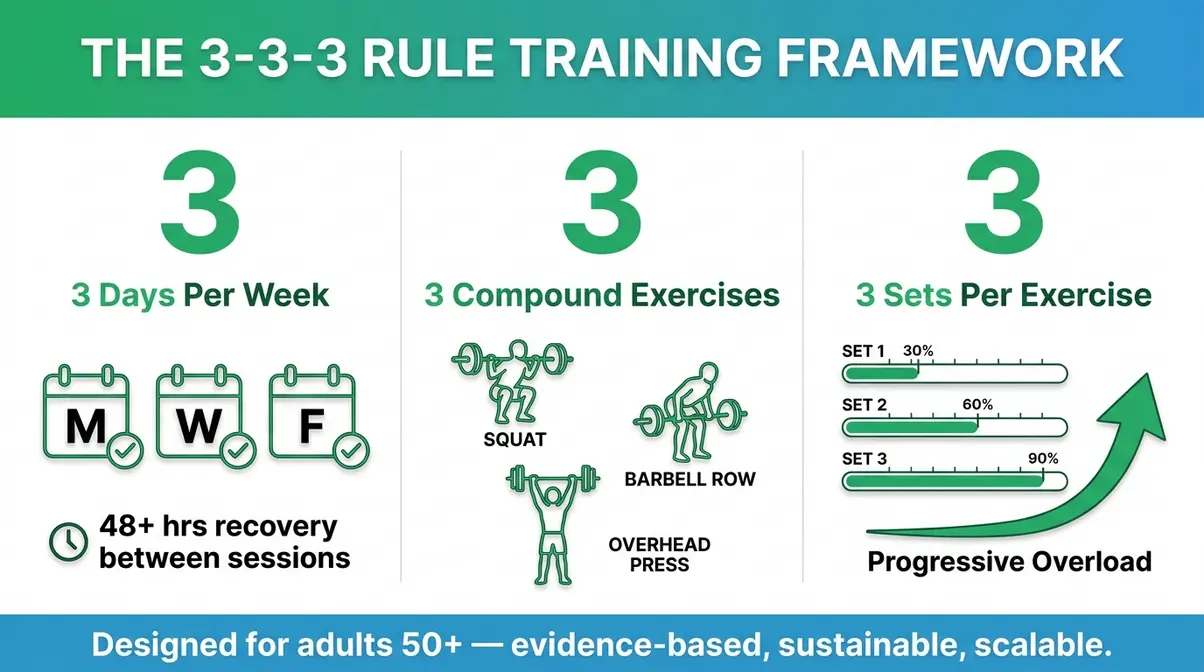
The 3-3-3 Rule Training Framework
The 3-3-3 Rule is a practical training framework gaining traction in exercise science communities as a sustainable, evidence-aligned approach for adults over 50. The principle is straightforward: 3 resistance training sessions per week, 3 compound exercises per session, 3 sets per exercise.
Here’s why this structure works for aging adults specifically:
- 3 sessions per week provides adequate training frequency while allowing 48+ hours of recovery between sessions — critical for older muscles that repair more slowly
- 3 compound exercises (movements like squats, rows, and presses that work multiple muscle groups simultaneously) maximize hormonal response and functional carry-over with minimal session time
- 3 sets per exercise sits within the evidence-supported range for hypertrophy (2–4 sets per exercise) without accumulating excessive fatigue
The 3-3-3 Rule is not a ceiling — it’s a floor. As fitness improves, you can add a fourth session, increase weight, or add accessory exercises. But for someone returning to training or managing age-related fatigue, it provides a manageable, non-overwhelming entry point with meaningful results.
Can a 70-Year-Old Still Build Muscle?
Yes — clinical studies consistently show that adults in their 70s and 80s can build measurable muscle mass through resistance training. A frequently cited study in the Journal of Applied Physiology found that adults aged 60–80 increased muscle cross-sectional area by 10–15% after 12 weeks of progressive resistance training. The National Institute on Aging confirms that strength training improves muscle mass, strength, and functional independence at any age. Recovery takes longer and protein needs are higher (2.0–2.2g per kg/day), but the biological pathway for growth remains open.
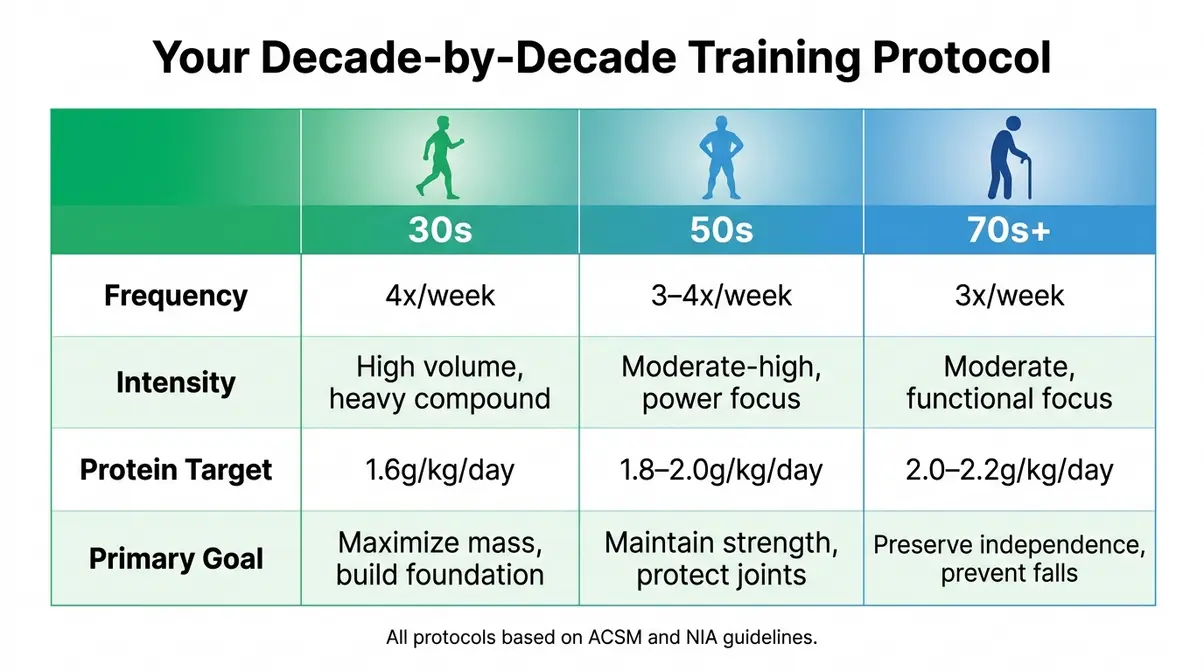
Age-Specific Training Protocols

Generic workout advice doesn’t serve you well when your biology is changing decade by decade. The protocols below are designed specifically for each life stage, grounded in current exercise science guidelines from the American College of Sports Medicine and the National Institute on Aging.
Evaluation Methodology: These protocols are drawn from ACSM resistance training guidelines for healthy older adults (2026), NIA strength training recommendations, and the peer-reviewed literature on progressive overload in aging populations. They represent evidence-based starting points, not individualized medical prescriptions.
Training in Your 30s: The Foundation
Your 30s are your best window to build a training foundation that will carry you through the decades ahead. Hormone levels, while beginning to decline, are still relatively high. Recovery is efficient. Your body responds well to volume.
Your 30s Protocol: Foundation Builder
Goal: Maximize muscle mass and establish movement patterns before anabolic conditions become more challenging.
Frequency: 4 sessions per week (Upper/Lower split or Push/Pull/Legs/Full Body)
Session Structure:
- Warm-up (5–10 min): Dynamic stretching + 2 light warm-up sets of your first exercise
- Compound Lifts (3–4 sets × 6–10 reps): Squat, deadlift, bench press, barbell row — rest 2–3 minutes between sets. These are your primary hypertrophy drivers.
- Accessory Work (2–3 sets × 10–15 reps): Lunges, dumbbell press, cable rows, lateral raises — rest 60–90 seconds
- Progressive Overload Target: Increase weight by 2.5–5 lbs every 2 weeks when you can complete all reps with good form
Protein Target: 1.6g per kg of bodyweight per day, distributed across 3–4 meals (minimum 30–40g per meal)
Key focus: Don’t skip mobility work. The movement quality you build now determines your training longevity in your 50s and 60s.
Training in Your 50s: Power & Protein
In your 50s, training smarter means adjusting volume and recovery without abandoning intensity. Research from The Conversation notes that “50-year-old muscles just can’t grow big like they used to” — but that’s about peak size, not about whether they grow at all (The Conversation). With the right approach, meaningful gains are very achievable. This makes optimal protein intake for muscle building absolutely essential.
Your 50s Protocol: Power and Protein
Goal: Maintain and build strength, protect joint health, and counteract anabolic resistance with protein timing.
Frequency: 3–4 sessions per week with mandatory 48-hour recovery between sessions
Session Structure:
- Warm-up (10–15 min): Longer than in your 30s — include joint mobility, foam rolling, and 3 light warm-up sets
- Power Emphasis (3 sets × 5–6 reps at higher intensity): Trap bar deadlift, goblet squat, dumbbell bench press — prioritize explosive intent (move the weight fast even if it isn’t fast)
- Hypertrophy Work (3 sets × 8–12 reps): Machine rows, leg press, cable chest press — machines reduce joint stress while maintaining muscle stimulus
- Core and Balance (10 min): Planks, single-leg stands, hip hinges — critical for fall prevention and functional strength
Protein Target: 1.8–2.0g per kg of bodyweight per day. Distribute across 4 meals. Consume 40–50g of protein within 30–60 minutes post-workout to maximize the narrowing anabolic window.
Key focus: Sleep 7–9 hours. Recovery is now a training variable, not a luxury.
Training in Your 70s: Safe Strength
The goal in your 70s shifts from aesthetics to functional independence and fall prevention — but the method is still resistance training. The evidence is unambiguous: the biggest risk to health in your 70s and 80s is not training too hard; it’s not training at all. These strength training benefits for older adults far outweigh the risks.
Your 70s+ Protocol: Functional Strength Builder
Goal: Preserve muscle mass, improve balance, reduce fall risk, and maintain independence.
Frequency: 3 sessions per week, every other day (e.g., Monday, Wednesday, Friday)
Session Structure (using the 3-3-3 Rule as your base):
- Warm-up (10–15 min): Gentle walking, chair-supported leg swings, shoulder circles
- Session A — Lower Body Focus:
- Sit-to-stand from chair (3 sets × 10–15 reps) — builds quad strength without joint stress
- Step-ups onto a low platform (3 sets × 8–10 reps per leg)
- Resistance band hip abduction (3 sets × 12–15 reps)
- Session B — Upper Body Focus:
- Seated dumbbell press (3 sets × 10–12 reps, light-to-moderate weight)
- Resistance band rows (3 sets × 12–15 reps)
- Wall push-ups or incline push-ups (3 sets × 8–12 reps)
- Session C — Full Body + Balance:
- Goblet squat with light dumbbell (3 sets × 8–10 reps)
- Dumbbell Romanian deadlift (3 sets × 10 reps)
- Single-leg balance hold (3 × 20–30 seconds per leg)
Protein Target: 2.0–2.2g per kg of bodyweight per day — at the high end, because anabolic resistance is most pronounced in this decade.
Key focus: Never train through sharp joint pain. Dull muscle fatigue is expected and fine. Sharp pain is a signal to stop and consult a physician.
Common Pitfalls and When to See a Doctor
Even with the right framework, certain mistakes consistently derail age-related muscle building efforts. Recognizing these patterns is as important as knowing the right protocols.
Mistakes That Accelerate Muscle Loss
Not eating enough protein is the single most common — and most correctable — mistake. Physical therapists and registered dietitians working with adults over 40 consistently report that most clients are consuming less than half the protein they need to support muscle maintenance, let alone growth. If you’re eating 0.8g per kg (the standard RDA), you’re likely leaving significant gains on the table.
Avoiding heavy compound lifts out of fear of injury is another common pitfall. Machines and light dumbbells have their place, but evidence suggests that multi-joint, heavier compound movements (squats, deadlifts, rows) produce the greatest hormonal response and hypertrophic stimulus. Proper form and gradual progression make these movements safe at any age.
Skipping recovery — including sleep, rest days, and stress management — undoes training gains faster than almost anything else. Muscles don’t grow during the workout; they grow during recovery. Cutting sleep to 5–6 hours actively elevates cortisol and suppresses growth hormone, creating exactly the hormonal environment you’re trying to avoid.
Staying in a caloric deficit for too long while trying to “lean out” simultaneously kills muscle-building efforts. Evidence suggests that muscle growth requires being at or near caloric maintenance — not a significant deficit. If fat loss and muscle gain are both goals, prioritize protein and resistance training first.
When Muscle Loss Is a Medical Issue
Most age-related muscle changes are gradual and respond well to lifestyle interventions. However, some scenarios warrant medical attention.
- See your physician if you notice:
- Rapid, unexplained muscle loss over weeks or months without changes in diet or activity
- Muscle weakness accompanied by fatigue, unexplained weight loss, or changes in bowel/bladder habits
- Severe muscle cramping or pain that is not linked to recent exercise
- Difficulty performing daily tasks (climbing stairs, rising from a chair) that appeared suddenly rather than gradually
- You are on a GLP-1 medication and are losing strength rapidly alongside weight
These symptoms may indicate underlying conditions — including thyroid disorders, vitamin D deficiency, neurological issues, or more serious diagnoses — that require evaluation beyond lifestyle change. Strength is not supposed to disappear quickly. If it does, that is a medical signal, not a training problem.
Frequently Asked Questions
Can you build muscle with high cortisol?
Yes, but chronically elevated cortisol significantly impairs muscle protein synthesis and accelerates muscle breakdown. Cortisol is catabolic — it breaks tissue down rather than building it up. Studies indicate that chronically high cortisol suppresses testosterone and growth hormone, creating a hormonal environment that actively works against muscle growth. Addressing cortisol through sleep (7–9 hours), keeping training sessions under 60 minutes, and managing psychological stress is as important as your workout program. Short-term cortisol spikes from exercise are normal and fine; it’s the chronic elevation that causes problems.
Can I gain muscle on GLP-1?
You can maintain and build muscle on GLP-1 medications, but only with intentional resistance training and high protein intake. Research cited by UCLA Health (2026) found that up to 25–39% of weight lost on semaglutide can come from lean muscle mass in the absence of structured exercise. The solution is concurrent resistance training and protein intake at 1.6–2.2g per kg of bodyweight daily.
Can you still gain muscle after 30?
Absolutely — muscle growth after 30 is well-documented and entirely achievable. Peak muscle mass occurs roughly between ages 20 and 30, after which a slow decline begins. However, this decline is only inevitable without training. Adults in their 30s who follow progressive resistance training programs with adequate protein intake consistently demonstrate measurable hypertrophy. The process may be slightly slower than in your early 20s due to beginning hormonal shifts, but the biological machinery for muscle growth remains fully functional throughout your 30s and beyond.
What is the 3-3-3 rule gym?
The 3-3-3 rule is a training framework designed for sustainable muscle building in aging adults: 3 resistance training sessions per week, 3 compound exercises per session, and 3 sets per exercise. This structure aligns with ACSM guidelines for older adults, providing sufficient training frequency and volume for hypertrophy while allowing adequate recovery time. It serves as a practical floor that can be progressively built upon as fitness improves.
What are the five signs of high cortisol?
The five most common signs of chronically elevated cortisol are: unexplained weight gain (especially around the abdomen), persistent fatigue despite adequate sleep, progressive muscle weakness, mood changes including irritability or anxiety, and slow or poor recovery from workouts. Cortisol is the body’s primary stress hormone and, when chronically elevated, actively breaks down muscle tissue while suppressing the anabolic hormones needed to rebuild it. If you recognize multiple signs, consult your physician — cortisol dysregulation can indicate underlying conditions (including Cushing’s syndrome) that require medical evaluation beyond lifestyle changes.
What hormone helps you build muscle?
Testosterone is the primary anabolic hormone for muscle growth, but growth hormone, insulin-like growth factor 1 (IGF-1), and insulin all play supporting roles. Testosterone signals muscle fibers to repair and hypertrophy after training stress, while growth hormone stimulates muscle protein synthesis and is released in pulses during deep sleep. Resistance training, adequate sleep, and stress management all support natural hormone optimization within healthy ranges.
Does muscle memory help older adults?
Yes, muscle memory significantly helps older adults regain lost strength faster than building it from scratch. The cellular adaptations from previous training remain in the muscle fibers, allowing for quicker hypertrophy when you resume lifting.
How long does it take to rebuild lost muscle?
The time it takes to rebuild lost muscle depends heavily on your prior training experience and current protein intake. Most older adults who follow a structured resistance program notice measurable strength improvements within 4 to 6 weeks. Visible muscle hypertrophy typically takes 8 to 12 weeks of consistent training. However, ensuring you consume adequate protein is critical to minimizing this recovery timeline.
Limitations and Considerations
Common Pitfalls to Avoid
The protocols and timelines in this article represent population-level research findings. Individual variation is significant — some people experience steeper hormonal declines earlier, while others maintain strong anabolic capacity well into their 60s. Applying a generic protocol without accounting for your training history, injury history, and current health status is a common mistake.
Specific scenarios where caution is warranted:
- Returning after a long break: Don’t begin where you left off. Muscle memory is real, but connective tissue (tendons, ligaments) adapts more slowly than muscle. Start at 50–60% of your previous working weights and build over 4–6 weeks.
- Chronic pain or orthopedic issues: The protocols above assume generally healthy joints. Anyone with diagnosed osteoarthritis, spinal stenosis, or recent joint surgery should work with a physical therapist to modify exercises before following any generic protocol.
- Rapid unexplained muscle loss: If you are losing muscle mass quickly without a clear dietary or training explanation, this is a medical issue — not a training problem. Consult your physician before modifying your exercise program.
When to Choose Professional Guidance
Generic articles — including this one — have real limits. An individualized assessment by a certified personal trainer (CSCS or CPT), registered dietitian, or physical therapist will always outperform a generic protocol for your specific body and goals.
Consider professional guidance if: you’re over 65 and new to resistance training, you have cardiovascular disease, diabetes, or osteoporosis, you’re currently on prescription medications that affect metabolism or muscle function, or you’ve been consistently training for 6+ months without measurable progress. According to the Mayo Clinic, you should seek immediate medical evaluation if you experience rapid, unexplained muscle wasting.
The Muscle Longevity Spectrum
Muscle capacity doesn’t fall off a cliff at a specific birthday. The Muscle Longevity Spectrum is the framework that replaces that fear with a more accurate picture: your ability to build and preserve muscle exists on a continuous, lifelong spectrum, shaped far more by what you do consistently than by the number on your driver’s license. If you’re still wondering at what age do muscles stop growing, the science is clear: they don’t.
The science is clear. Adults in their 30s, 50s, and 70s all retain the biological capacity for meaningful muscle growth. Testosterone declines, anabolic resistance increases, and recovery slows — but none of these changes close the door on progress. They change the combination required to open it: more protein, smarter programming, better sleep, managed stress.
Start with the protocol that matches your decade. Follow the 3-3-3 Rule if you’re returning to training or need a sustainable structure. Hit your protein target every day — this single variable may be the highest-leverage change most adults over 40 can make. And if you’re on a GLP-1 medication, make resistance training a non-negotiable part of that conversation with your doctor.
Your training age — how long you’ve trained consistently and how well you’ve recovered — matters more than your calendar age. The best time to start was years ago. The second-best time is this week.
Reviewed for medical accuracy by a certified exercise science professional. This article cites Tier 1–2 sources including the National Institute on Aging, Harvard Health Publishing, the American College of Sports Medicine, and peer-reviewed publications in PMC.
