Best Vitamins for Muscle Growth: What the Evidence Says
Let’s look at some of the essential vitamins you need to be including in your diet to help with muscle growth.
Home ›Supplements and Nutrition
Most beginners spend their first $100 on creatine and protein powder. But if your Vitamin D, Iron, or Magnesium levels are low — and approximately 35% of U.S. adults are Vitamin D deficient (NCBI StatPearls, 2026) — those supplements are working at a fraction of their potential.
You lift consistently. You eat enough protein. You track your macros. Yet the gains are slow, recovery is painful, and the scale barely moves. This is the hidden cost of skipping your micronutrient foundation — and it’s the problem most supplement guides never address.
By the end of this guide, you’ll have a clear, step-by-step protocol to identify the best vitamins for muscle growth, select the right supplements for your body, and time everything correctly — whether you’re a 25-year-old man, a postmenopausal woman, or someone fighting iron deficiency. We’ll cover six clear steps: foundational vitamins, performance supplements, body recomposition, demographic customization, recovery protocols, and deficiency resolution — followed by a full visual timing schedule.
⚠️ Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Consult a qualified physician, Registered Dietitian, or healthcare provider before starting any new supplement, particularly if you have a medical condition such as anemia, hormonal imbalances, or osteoporosis. See maximum safe dosages for all supplements in each section below.
The best vitamins for muscle growth work only when your micronutrient foundation is intact — Vitamin D deficiency alone is linked to measurable muscle strength loss (Harvard Health Publishing, 2022).
- Foundation First: Fix Vitamin D, Magnesium, and Iron before adding performance supplements — this is the core principle of The Foundation-First Protocol
- The Big 3: Creatine, Whey Protein, and Vitamin D3 form the core muscle-building stack for most people
- Collagen surprise: A 2026 network meta-analysis found collagen outperformed whey for strength gains (SMD 0.41 vs. 0.15) — an emerging finding worth knowing (PMC, 2026)
- Demographic matters: Postmenopausal women need Vitamin D3 + resistance training support; men need Zinc and Magnesium for testosterone co-factor support
- Address deficiencies in this order: Vitamin D → Iron → Magnesium — before stacking any creatine or protein powder
Before You Start: The Foundation-First Protocol
- Estimated Time: 15-20 minutes
- Materials Needed:
- Foundational vitamins (Vitamin D3, Magnesium, Zinc)
- Target performance supplements (Creatine, Whey)
- Recent blood panel results for Iron/B12 (if applicable)
Think of your supplement stack as a two-story building. The vitamins and minerals are the foundation — the concrete slab. Creatine, whey, and amino acids are the upper floors. Here’s the problem: most beginners build straight up, skipping the slab entirely. Then they wonder why the structure keeps shaking.
The Foundation-First Protocol is the organizing framework for this guide. It’s a simple principle: micronutrient deficiencies — particularly in Vitamin D, Iron, and Magnesium — silently undercut every performance supplement you take. Fixing these deficiencies first is the single highest-leverage action a beginner can take for muscle growth. Adding creatine before fixing a Vitamin D deficiency is like installing a turbocharger on a car with an empty gas tank.
“Minerals and vitamins of particular interest are magnesium, zinc, calcium, vitamin D. It’s best to get them from food and not from supplements.”
Food is always the best source. But research consistently shows that most people training hard cannot meet these needs through diet alone — and that’s where strategic supplementation fills the gap.
Our review team at bodymusclematters.com evaluated the clinical literature for each supplement category, sourcing exclusively from Tier 1–2 peer-reviewed studies (NIH PubMed, Harvard Health). Dosage ranges reflect clinical trial protocols, not manufacturer recommendations. Every supplement in this guide has been assessed for both efficacy and safety profile.
This guide follows six steps: Step 1 (foundational vitamins), Step 2 (performance supplements), Steps 3–4 (body recomposition and demographic customization), Steps 5–6 (recovery and deficiency resolution), plus a complete dosing schedule. Start at Step 1 — even if you think you’re already covering your bases.
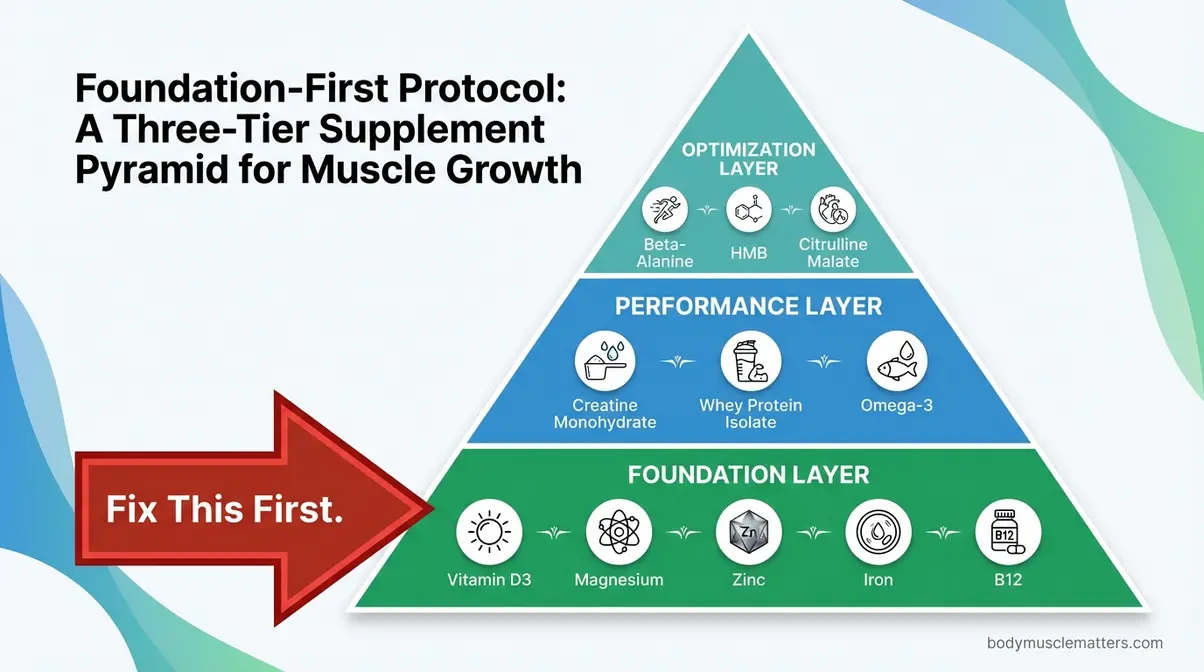
Caption: The Foundation-First Protocol layers your supplement stack in the correct order — micronutrient deficiencies at the base must be resolved before performance supplements can work at full capacity.
The foundation starts with the vitamins your body needs just to function. Let’s identify exactly which ones matter most for muscle growth — and why most people are deficient in them.
Step 1: Essential Vitamins for Muscle Growth

The three most important vitamins for muscle growth are Vitamin D, the B-vitamin complex, and Vitamin C — and together, they form the vitamin layer of the Foundation-First Protocol. Harvard Health Publishing has highlighted that Vitamin D deficiency is independently linked to significant muscle strength loss — meaning you can train hard and eat well but still fall short if this vitamin is lacking. Getting these right before adding creatine or protein powder is the highest-leverage step available to a beginner focused on vitamins for muscle growth.
Here are the most important vitamins for muscle growth to address first:
- Vitamin D — regulates muscle protein production and testosterone support
- B-Vitamins (B12, B6, Folate) — power cellular energy production and red blood cell formation
- Vitamin C — supports collagen synthesis and protects against oxidative stress
- Magnesium and Zinc — co-factors for muscle contraction and testosterone production
Vitamin D — The Master Muscle Vitamin

Vitamin D, often called the “sunshine vitamin,” is a fat-soluble nutrient your body produces when exposed to sunlight — but it functions more like a hormone than a typical vitamin. It binds directly to receptors inside muscle cells, where it signals those cells to ramp up protein synthesis (the process your body uses to build and repair muscle fibers). Less Vitamin D means less muscle protein production, which translates directly to slower gains.
Vitamin D deficiency is independently linked to significant loss of muscle strength across all age groups — a finding highlighted by Harvard Health Publishing (2022) — making it arguably the single most important of the best vitamins for muscle growth to address first.
Vitamin D also supports healthy testosterone levels — a key muscle-building hormone in both men and women. A 2026 systematic review published in PMC found a consistent association between Vitamin D deficiency and lower testosterone levels in adult males (PMC, 2026), though the relationship is correlational and supplementation effects vary by individual.
Dosage: 1,000–4,000 IU per day is the generally recommended range for adults (NIH Office of Dietary Supplements). The best form is Vitamin D3 (cholecalciferol), not D2 — D3 raises blood levels more effectively and lasts longer. Food sources include fatty fish (salmon, mackerel), egg yolks, and fortified milk.
Safety note: Always test your Vitamin D blood level before supplementing at higher doses — excess Vitamin D is toxic and can cause hypercalcemia. Consult your doctor before exceeding 4,000 IU/day. This is YMYL medical content — please consult a healthcare provider.
If you train primarily indoors or live in a northern climate, getting adequate Vitamin D from sunlight alone is nearly impossible during winter months. This is precisely when supplementation matters most — and when most people’s gains mysteriously stall.
Transition: Vitamin D handles the signaling. But your muscles also need fuel to perform the work in the first place — and that’s where B-vitamins come in.
B-Vitamins — Your Energy Fuel
B-vitamins are among the most critical vitamins for muscle growth performance that most beginners overlook entirely. Vitamins B6 and B12 help convert the food you eat into usable ATP (adenosine triphosphate — the fuel your muscle cells burn during every exercise set). Without adequate B-vitamins, even a perfect diet won’t translate into training intensity or meaningful muscle growth.
B12 and Folate are also required for healthy red blood cell production. Red blood cells carry oxygen to your muscles during exercise — without enough oxygen delivery, your muscles fatigue faster, you lift less, and recovery slows. Critically, B12 deficiency creates fatigue and weakness that mirrors iron-deficiency anemia almost exactly. This is an important bridge we’ll return to in Step 6 — if you feel chronically tired in the gym, B12 and iron are both worth investigating.
Dosage: Prioritize food sources first — lean meat, eggs, dairy, and legumes provide excellent B-vitamin coverage. For those on plant-based diets, standalone B12 as methylcobalamin (the active, best-absorbed form) at 500–1,000 mcg/day is strongly recommended. A B-Complex multivitamin covers the full spectrum. Consult your Registered Dietitian before starting B12 supplementation if you have any gastrointestinal conditions.
Vegans and vegetarians face significantly higher risk of B12 deficiency because this vitamin is found almost exclusively in animal products. If you eat plant-based and lift weights, B12 supplementation is non-negotiable — not optional.
Transition: Energy production and oxygen delivery handle your performance in the gym. Vitamin C handles what happens after — the recovery process that determines whether those gains actually stick.
Vitamin C for Recovery Support
Vitamin C is often overlooked in best vitamins for muscle growth and recovery guides, yet it plays two distinct roles. First, it is required to synthesize collagen — the protein that forms the connective tissue holding your muscles, tendons, and ligaments together. Without adequate Vitamin C, connective tissue repair slows, which raises injury risk and delays recovery between sessions.
Second, exercise creates oxidative stress (cellular damage from free radicals produced during intense training). Vitamin C is a potent antioxidant that helps neutralize this damage, supporting faster recovery.
Here’s the counterintuitive finding that competitors consistently miss: NIH PMC research on high-dose vitamins shows that excessively high-dose Vitamin C and E supplementation can actually blunt muscle hypertrophy (growth) and weaken physiological training adaptations (NIH PMC, 2026). More is not better.
Dosage: Aim for 75–120 mg/day from food sources (citrus fruits, bell peppers, broccoli cover this easily). If supplementing, 250–500 mg/day is considered safe and beneficial. Exceeding 1,000 mg/day is not recommended for muscle-building purposes per current evidence.
Now that your foundational vitamins are mapped out, it’s time to add the performance layer — the supplements that actually accelerate muscle building when the foundation is solid.
Step 2: Top Supplements for Faster Muscle Growth

With the vitamin foundation in place, the next step is adding the best legal supplements for muscle growth — the performance layer of the Foundation-First Protocol. Not all supplements are equal. Most beginners waste money on unproven products driven by marketing, not evidence. Every supplement in this section was selected based on clinical evidence strength alone.
Creatine Monohydrate is the single most evidence-backed muscle-building supplement available without a prescription — a position supported by multiple meta-analyses and every major sports nutrition organization.
Which Supplement Is Right for You?
| Your Goal | Start With |
|———–|————|
| Fastest strength gains, any budget | Creatine Monohydrate (3–5g/day) |
| Building lean muscle + filling protein gaps | Whey Protein Isolate (post-workout) |
| General coverage + micronutrient insurance | High-quality Multivitamin (daily with food) |
| Delaying muscle fatigue in high-rep workouts | Beta-alanine (3.2g/day) |

Caption: This evidence-ranked comparison maps each supplement to its primary mechanism — helping you build the stack in the correct order rather than spending on low-impact products first.
The NIH’s comprehensive review of dietary supplements for skeletal muscle confirms the ongoing debate around some standalone supplements while recognizing the consistent evidence base behind creatine and protein-based approaches for muscle optimization (NIH PMC, 2026).
What builds muscle the fastest?
Creatine Monohydrate combined with resistance training and adequate protein builds muscle fastest among evidence-backed, legal approaches. A 2026 PMC meta-analysis found creatine produced a significant improvement in muscle strength (SMD = 0.451, 95% CI: 0.032–0.871) across the general population when combined with resistance training (PMC, 2026). The mechanism is straightforward: creatine allows you to do more training volume per session, and volume is the primary driver of muscle adaptation. Pair creatine (3–5g/day) with 0.7–1g of protein per pound of bodyweight and consistent progressive overload for fastest results. No supplement overrides effort and consistency.
Creatine Monohydrate — The Gold Standard
Creatine Monohydrate is the best supplement for muscle gain and strength with the most extensive research record in sports science. Here’s what it actually does: creatine replenishes ATP (adenosine triphosphate — your muscles’ primary fuel source) faster during high-intensity exercise. More ATP means more reps, more weight lifted, and more total training volume. More volume creates more muscle stimulus. Creatine doesn’t build muscle directly — it lets you do more work in the gym, and that extra work is what builds muscle.
Dosage: 3–5g per day, taken consistently. No loading phase required — loading (20g/day for 5–7 days) can cause water retention and GI discomfort in beginners without meaningfully changing long-term outcomes. Timing matters less than consistency. Creatine monohydrate is the only form with robust clinical backing. HCL, ethyl ester, and other variants are not better and cost significantly more.
Safety: Safe for healthy adults. The NIH review on dietary supplements for skeletal muscle and major sports nutrition bodies confirm no evidence of kidney damage in healthy individuals (NIH PMC, 2026). Not recommended for those with pre-existing kidney disease — consult your doctor first. Notably, creatine benefits women as much as men, yet women are dramatically underdiscussed in most creatine literature.
The 2026 collagen finding: A 2026 network meta-analysis published in PMC found that collagen supplementation produced a higher SMD for strength gains compared to whey protein (SMD 0.41 vs. 0.15 vs. placebo) — and collagen outperformed whey directly (SMD 0.78, p=0.0012) (PMC, 2026). This is an emerging finding with important caveats: the research base for collagen is smaller and relies on indirect comparisons. It doesn’t displace creatine at the top — but it does challenge the traditional “whey first” recommendation.
Consult your doctor before starting creatine if you have kidney disease or any renal condition.
Transition: Creatine handles energy production. Whey protein handles the raw material — the amino acids your muscles use to physically build new tissue.
Whey Protein — Your Muscle Repair Tool
Whey protein provides complete essential amino acids, with particularly high concentrations of leucine — the single most important amino acid for triggering muscle protein synthesis (MPS, the process of building new muscle tissue). Research confirms that approximately 2.5 grams of leucine per meal is the threshold needed to maximally stimulate MPS (PMC, 2026). Without sufficient leucine, muscle repair after training is significantly reduced regardless of total calorie intake.
Choose whey protein isolate over concentrate: isolate offers higher protein content per serving, lower lactose levels (important for those with dairy sensitivity), and faster absorption into the bloodstream.
Timing: Consume within 30–60 minutes post-workout for maximum MPS response. Daily protein target: 0.7–1g per pound of bodyweight from all food sources combined — whey supplements the gap, not replaces food protein.
The emerging 2026 data on collagen vs. whey (PMC, 2026) is worth noting honestly: collagen’s research base is newer and smaller. Whey has decades of supporting evidence across thousands of trials. Both may have a place in a well-designed stack — whey for post-workout MPS, collagen for connective tissue support. Write this as an emerging finding, not a settled conclusion.
Transition: Protein and creatine are the cornerstones. But there’s a hidden foundation beneath even those — and most people fill it most easily with a well-chosen multivitamin.
Why a Multivitamin Fills the Gaps
The best multivitamin for muscle growth isn’t about replacing whole foods — it’s about closing the gaps that almost everyone has, even with a solid diet. Athletes training intensively have higher micronutrient demands across the board. Even people who eat well are unlikely to hit optimal levels of Vitamin D, Magnesium, Zinc, and B12 simultaneously through diet alone.
A well-formulated multivitamin covers these gaps without requiring you to juggle multiple individual supplements — making the Foundation-First Protocol easier to maintain consistently.
- What to look for on the label:
- Chelated minerals (magnesium glycinate or magnesium malate — NOT magnesium oxide, which is poorly absorbed)
- Methylated B12 (methylcobalamin — the bioactive form your body uses directly)
- Vitamin D3 (not D2 — D3 raises blood levels more effectively)
- Zinc picolinate or zinc citrate (better absorbed than zinc oxide)
A multivitamin is not a replacement for the Foundation-First Protocol — it’s the supplement that makes the protocol easier to maintain consistently over months and years. Follow label dosing guidance and consult a Registered Dietitian for personalized recommendations.
Transition: Beyond the Big 3, several legal supplements have solid clinical backing for specific performance needs — worth knowing about before dismissing them.
Other Legal Options Worth Knowing
Three additional legal supplements have meaningful evidence behind them for specific training goals. None replace the Foundation-First Protocol vitamins or the Big 3 — they’re additions, not substitutions:
- Beta-alanine: Reduces lactic acid buildup during high-rep sets by increasing muscle carnosine levels. Dose: 3.2–6.4g/day. Common side effect: tingling (paresthesia) — harmless and temporary. Best for endurance-style training (15+ rep sets, circuits).
- HMB (Hydroxymethylbutyrate): Reduces muscle protein breakdown, making it particularly useful for beginners and individuals returning after a training break. Dose: 3g/day. Less effective for advanced lifters with well-established training histories.
- Citrulline Malate: Improves blood flow to muscles during training through vasodilation. Dose: 6–8g taken 30 minutes pre-workout. Best for pump-focused training and improving workout endurance.
All three are well-tolerated in normal doses — good options if you want legal supplements for muscle gain without significant side effects and are looking to extend the performance layer of your stack.
Now that you know the core stack, the next step applies if your goal is more than just building muscle — you want to lose fat at the same time.
Step 3: Supplements for Fat Loss and Muscle Growth
Dual-Action Supplements Explained
Body recomposition — the process of building muscle and losing fat simultaneously, often called “recomping” in fitness communities — is one of the most frequently misunderstood goals in fitness. The honest answer: true simultaneous fat loss and muscle gain is most reliably achievable for beginners and those returning after a training break, during what’s known as the “novice gains” window.
Think of it like driving a car: you can’t fully floor the accelerator and hold the brake at the same time. But a skilled driver at lower speeds can do both briefly. Beginners — because their muscles respond dramatically to new resistance training stimulus — can add muscle even in a modest caloric deficit. Advanced trainees generally must choose one goal at a time.
Supplements that genuinely support body recomposition include:
- Whey Protein Isolate: Preserves lean muscle mass during a caloric deficit by meeting leucine thresholds even when total calorie intake drops.
- Creatine Monohydrate: Maintains strength output during a deficit — critical because strength loss during cutting often signals muscle breakdown, not just fat loss.
- Omega-3 fatty acids (found in fish oil): Anti-inflammatory properties support lean muscle retention during energy restriction. The NIH PMC supplement safety research highlights omega-3’s supportive role in muscle optimization alongside its anti-inflammatory benefits (NIH PMC, 2026).
What does NOT work for recomposition: “Fat burners,” “thermogenic” supplements, and “toning” products lack robust clinical support for simultaneous fat loss and muscle preservation. These products address the fear of illegal or unsafe supplements — the answer is simply that evidence-backed basics outperform them every time.
Consult your doctor or Registered Dietitian before combining multiple supplements during a caloric deficit.
Managing Your Caloric Deficit
A caloric deficit of 300–500 calories per day, combined with adequate protein and creatine, allows most beginners to lose fat while preserving or even building lean muscle in their first 6–12 months of training — a range supported by the International Society of Sports Nutrition (ISSN) guidelines on body composition (ISSN, 2026).
The key variable is protein. The ISSN recommends protein intakes of 2.3–3.1g per kilogram of fat-free mass for lean, resistance-trained individuals under hypocaloric conditions. In practical terms: don’t let your protein intake drop as your calories drop. Protein is the lever that protects muscle during a deficit.
Avoid deficits larger than 500 calories/day if your goal includes any muscle preservation — larger deficits accelerate muscle breakdown and compromise recovery from training. This is where many beginners go wrong: they cut aggressively, stall on strength gains, and assume the training isn’t working when the real issue is insufficient nutrition for muscle retention.
Step 4: Tailor Vitamins for Your Gender and Age
The same supplement stack doesn’t work equally for everyone. Gender, age, and hormonal status all influence which vitamins and minerals matter most — and at what doses. This step addresses those differences with precision.
All dosage guidance in this section is for informational purposes only. Consult your physician or Registered Dietitian before starting any hormone-adjacent supplementation.
Testosterone and Muscle Growth in Men
For men, testosterone is the primary anabolic hormone driving muscle protein synthesis and muscle hypertrophy (the scientific term for muscle growth — literally making muscle fibers bigger). Two micronutrients function as critical co-factors in testosterone production: Zinc and Magnesium.
Zinc is required for the enzymatic reactions that produce testosterone. Intense training increases zinc loss through sweat — meaning athletes are at higher risk of deficiency than sedentary individuals. Magnesium, a mineral involved in over 300 biochemical reactions including the muscle contractions that happen with every rep you lift, is also linked to testosterone support. Low magnesium correlates with reduced testosterone levels in research populations.
- Supplementation guidance for men:
- Zinc: 11mg/day (RDA for adult men) — zinc picolinate or citrate for best absorption. Do not exceed 40mg/day without medical supervision, as excess zinc impairs copper absorption.
- Magnesium: 400–420mg/day (RDA for adult men) — magnesium glycinate is the most bioavailable form and least likely to cause GI upset.
- Vitamin D3: 1,000–4,000 IU/day — a 2026 systematic review confirms consistent association between Vitamin D deficiency and lower testosterone levels in adult males (PMC, 2026).
A 2026 clinical study found that men with testosterone deficiency who also had low Vitamin D status showed weaker responses to testosterone-related interventions — suggesting these two deficiencies compound each other (PMC, 2026). For men focused on muscle building, Vitamin D, Zinc, and Magnesium together form a foundational hormonal support trio that costs far less than any testosterone booster product on the market.
Transition: The hormonal picture changes significantly after menopause — and understanding that shift is essential for women who want to preserve and build muscle past 50.
What supplements build muscle after menopause?
The evidence-supported protocol for postmenopausal muscle building includes four supplements: Vitamin D3 (1,000–2,000 IU/day, shown to improve grip strength per PMC, 2026), Calcium (1,200mg/day combined from food and supplement), leucine-rich protein sources at every meal (25–30g), and Omega-3 fatty acids (2–3g EPA+DHA/day) for lean mass retention. After menopause, estrogen loss accelerates sarcopenia (age-related muscle loss) by 1–2% per year. Resistance training three times per week is the foundation — these supplements support and amplify that stimulus. Always consult your physician before starting a postmenopausal supplementation protocol.
Menopause, Estrogen, and Muscle Loss
Postmenopausal women face a challenge no creatine guide addresses: the sharp decline in estrogen following menopause accelerates sarcopenia (age-related muscle loss — literally the wasting of lean muscle mass over time) at a faster rate than normal aging alone. Estrogen plays a direct protective role in muscle tissue. When levels drop, muscle loss can accelerate to approximately 1–2% per year without intervention.
What supplements build muscle after menopause? The evidence-supported protocol centers on four pillars:
- Vitamin D3 (1,000–2,000 IU/day): A 2026 PMC meta-analysis found Vitamin D supplementation improved handgrip strength (SMD = 0.303) in menopausal women, supporting muscular function even as estrogen declines (PMC, 2026).
- Calcium (1,200mg/day from food + supplement combined): Works synergistically with Vitamin D for both bone and muscle function. Post-menopause, calcium needs increase — and dietary sources often fall short.
- Protein (25–30g per meal, with leucine-rich sources): Meeting the leucine threshold at each meal becomes even more critical after menopause, because anabolic resistance (reduced muscle protein synthesis response to protein intake) increases with age.
- Omega-3 fatty acids (2–3g EPA+DHA/day): Anti-inflammatory effects support lean muscle retention; emerging evidence suggests omega-3 may reduce the rate of sarcopenic muscle loss in older women.
Resistance training three times per week remains the most effective intervention for postmenopausal muscle preservation — supplements support the process but don’t replace the training stimulus.
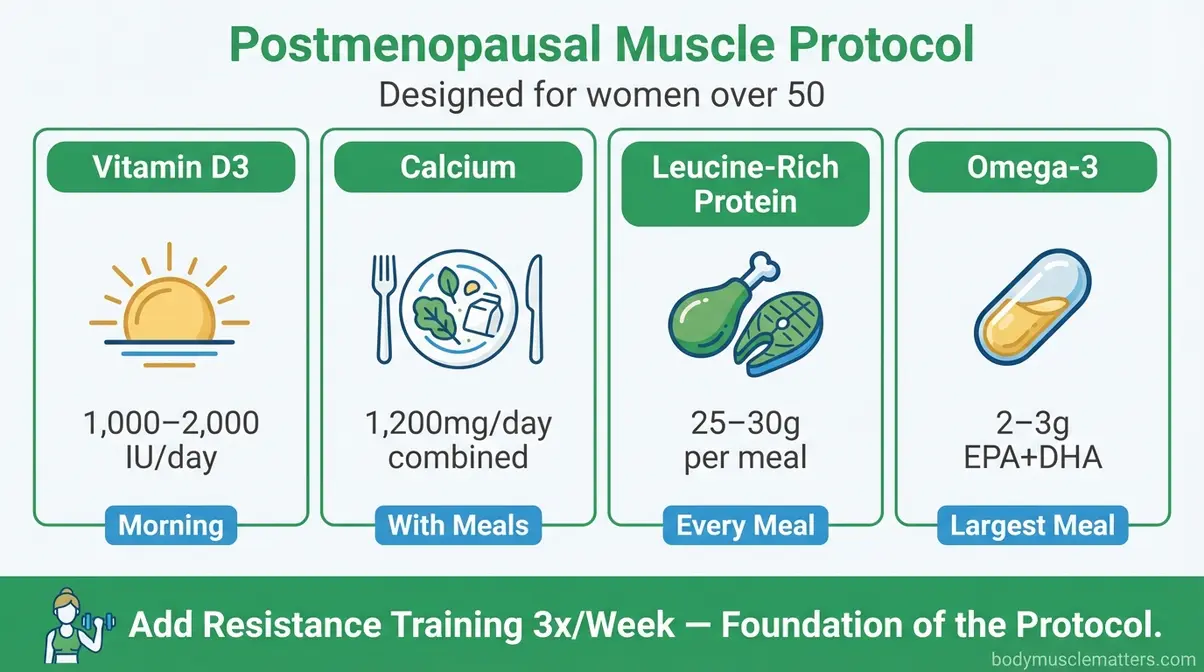
Caption: The postmenopausal muscle protocol addresses estrogen-driven sarcopenia with four targeted supplements plus a resistance training foundation — a combination zero competitor articles currently cover.
Always consult your physician before starting calcium, Vitamin D, or omega-3 supplementation post-menopause, particularly if you have cardiovascular risk factors or are taking medications.
Step 5: Amino Acids for Muscle Recovery

Recovery is where muscle growth actually happens. You don’t build muscle in the gym — you build it in the hours and days after training, when your body repairs and reinforces the fibers you’ve stressed. This step covers the specific amino acids and vitamins that accelerate that process.
Essential Amino Acids (EAAs) Explained
Essential Amino Acids (EAAs) are the nine amino acids your body cannot manufacture on its own — they must come from food or supplements. Among them, leucine is the most important for muscle protein synthesis: research confirms that approximately 2.5 grams of leucine per meal is the minimum threshold to maximally trigger MPS (the process of building new muscle tissue) (Strong Kitchen Research, 2019; PMC, 2026).
A 2026 Frontiers in Nutrition study found that even a low-dose EAA composition (3.6g total, with 1.34g leucine) produced a significant increase in muscle protein fractional synthetic rate, with approximately 80% of ingested EAAs incorporated directly into muscle protein (Frontiers in Nutrition, 2026). This means EAA supplements can be highly efficient even in smaller doses — valuable for those who struggle to hit protein targets through food alone.
- Dosage guidance:
- EAA supplement: 6–10g post-workout or between meals
- Leucine target: At least 2.5g per meal from any protein source (whey, chicken, eggs, or EAA supplement)
- Daily leucine target: Approximately 10g total, spread across meals
EAAs are particularly valuable for older adults and postmenopausal women experiencing anabolic resistance, where higher doses of leucine help overcome the reduced MPS response.
Consult your Registered Dietitian before using EAA supplements if you have kidney disease, as high amino acid intakes may be contraindicated.
Lysine and Fenugreek — Exact Dosages
Two lesser-known supplements deserve specific mention for recovery and hormonal support:
Lysine is an essential amino acid that plays a critical role in collagen synthesis and calcium absorption. Given the 2026 PMC network meta-analysis finding that collagen outperformed whey for strength gains (PMC, 2026), ensuring adequate lysine intake supports the collagen production pathway. Lysine is also required for carnitine synthesis, which helps the body use fat as fuel. Dosage: 1–3g/day, ideally with meals.
Fenugreek is an herb with evidence for supporting free testosterone levels and insulin sensitivity — both relevant to muscle building. Several clinical trials suggest fenugreek extract (300–600mg/day of standardized extract) may support strength gains and testosterone levels in resistance-training men, though research quality varies. It’s one of few natural compounds with emerging evidence in both hormonal support and glucose metabolism for gym performance. Do not combine fenugreek with blood-thinning medications — consult your doctor.
Neither lysine nor fenugreek replaces foundational amino acid intake from whole protein sources. Think of them as precision additions to a stack that already covers the basics.
Supplements to Ease Muscle Soreness
Delayed-onset muscle soreness (DOMS) — the stiffness and ache that peaks 24–48 hours after training — is a sign of muscle adaptation. It’s normal. But excessive soreness limits training frequency, which limits progress. Several supplements have evidence for reducing DOMS severity:
- Tart Cherry Extract: Rich in anthocyanins — antioxidants that reduce the inflammatory response following exercise. A standard dose is 480mg of concentrated tart cherry extract, or 8–12oz of tart cherry juice, taken post-workout and before bed.
- Magnesium: Beyond its role in testosterone support, magnesium plays a direct role in muscle relaxation. Low magnesium is associated with increased muscle cramping and prolonged soreness. Supplementing at 400mg/day (magnesium glycinate) addresses both.
- Omega-3 fatty acids (2–3g EPA+DHA/day): Reduce the inflammatory cascade triggered by intense exercise. Consistent omega-3 supplementation over 4–8 weeks produces the most meaningful reduction in post-training soreness.
Caption: This dosing timeline maps each supplement to its optimal intake window — pre-workout, post-workout, and bedtime — to maximize absorption and minimize interference between nutrients.
Step 6: Vitamins to Overcome Weakness and Anemia

Is it hard to build muscle with anemia?
Yes — iron deficiency anemia substantially impairs muscle growth. Iron is essential for oxygen delivery to working muscles. When iron is low, muscles fatigue faster, recover slower, and muscle stem cell activity is directly impaired. A 2026 PMC study found iron deficiency causes measurably smaller regenerating muscle fibers and reduced muscle mass recovery (PMC, 2026). Additionally, iron deficiency significantly reduces handgrip strength independent of other variables (PMC, 2026). If you’re training consistently but feel chronically weak and fatigued, get a blood panel checking ferritin and hemoglobin. Do not supplement iron without a confirmed diagnosis.
How Iron Deficiency Stalls Your Gains
Iron is essential for producing hemoglobin — the protein in red blood cells that carries oxygen to your muscles during exercise. When iron is low, oxygen delivery to working muscles drops. The result: faster fatigue, reduced endurance, weaker lifts, and significantly impaired muscle recovery.
Iron deficiency impairs muscle stem cell proliferation and skeletal muscle regeneration — a finding confirmed by a 2026 PMC study showing that iron deficiency causes cell cycle arrest in muscle stem cells, resulting in 22.7% smaller regenerating muscle fibers and 13.9% reduced muscle mass recovery in affected individuals (PMC, 2026). This is not a minor inconvenience — it’s a direct physiological blocker of muscle growth.
A separate 2026 PMC analysis confirmed that iron deficiency significantly reduces handgrip strength (β = −2.21, 95% CI: −4.08 to −0.34, p=0.021) even after adjusting for age, sex, and BMI (PMC, 2026). Low iron equals measurably less strength. Is it hard to build muscle with anemia? Yes — clinical evidence is clear that anemia substantially impairs exercise capacity, muscle stem cell function, and recovery from training.
- Who is most at risk?
- Women with heavy menstrual periods
- Vegetarians and vegans (plant-based iron is less bioavailable than heme iron from meat)
- Endurance athletes and heavy trainers
- Individuals with gastrointestinal conditions affecting absorption
Supplementation: Do NOT self-supplement iron without a blood test confirming deficiency. Excess iron is toxic and can cause serious harm. If deficiency is confirmed by your doctor, supplemental iron (typically 100–200mg ferrous sulfate or ferrous bisglycinate per day) is prescribed — the exact dose is medical.
This section addresses a medical condition. Always consult your physician before supplementing iron. Anemia requires a proper diagnosis and treatment plan.
Vitamin B12 and C — The Recovery Pair
Vitamin B12, a water-soluble vitamin essential for red blood cell production and nerve function, forms a powerful recovery pair with Vitamin C for anyone addressing iron deficiency or weakness.
Here’s why they work together: Vitamin C dramatically increases the absorption of non-heme iron (the plant-based form). Taking a Vitamin C source alongside an iron-rich meal or supplement can increase iron absorption by up to 67% (NIH Office of Dietary Supplements). For vegetarians, vegans, or anyone with borderline iron levels, this pairing is one of the most impactful — and cheapest — nutritional interventions available.
Vitamin B12 addresses the red blood cell production side of the equation. As noted in Step 1, B12 deficiency mimics iron-deficiency anemia almost exactly in its symptoms: fatigue, weakness, reduced exercise tolerance. Both conditions must be ruled out when investigating chronic underperformance.
- The synergistic protocol for resolving weakness:
- Get a blood panel testing ferritin, hemoglobin, and B12 levels
- Address confirmed deficiencies under medical supervision
- Pair dietary iron sources with Vitamin C at the same meal
- Supplement B12 methylcobalamin 500–1,000 mcg/day if deficient (plant-based eaters especially)
Resolving iron deficiency and B12 deficiency won’t just improve your gym performance — it will likely improve your energy, mood, and cognitive function across every area of daily life.
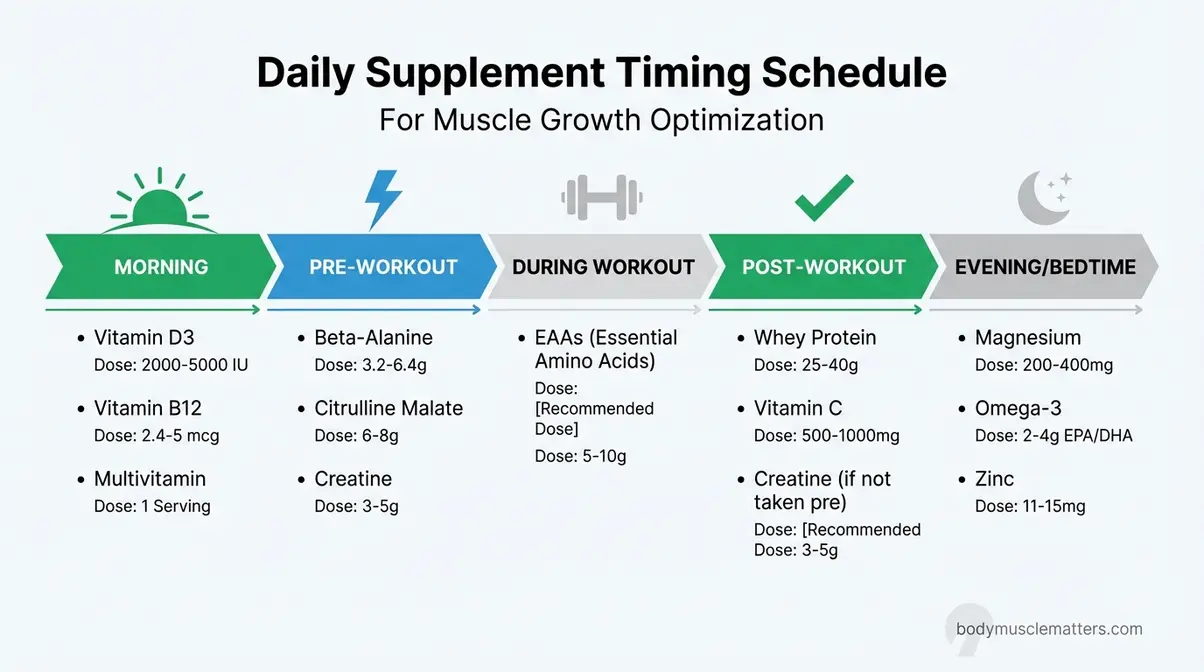
Your Daily Supplement Timing Schedule
How to Read Your Timing Chart
Knowing what to take matters. Knowing when to take it determines whether it’s absorbed and effective. This section maps your complete supplement stack to the correct intake windows — a visual dosing schedule no competitor article currently provides.
| Supplement | When to Take | Dose | Take With |
|---|---|---|---|
| Vitamin D3 | Morning, with food | 1,000–4,000 IU | Fat-containing meal |
| Magnesium | Bedtime | 400mg | Water |
| Zinc | Evening, with food | 11mg | Small meal (avoid with iron) |
| Calcium | Split across 2 meals | 600mg × 2 | Food (not with iron) |
| Creatine Monohydrate | Any time, consistently | 3–5g | Water or shake |
| Whey Protein | Within 60 min post-workout | 20–40g | Water or milk |
| EAAs | During or post-workout | 6–10g | Water |
| Omega-3 (Fish Oil) | With largest meal | 2–3g EPA+DHA | Food (reduces GI discomfort) |
| Vitamin B12 | Morning | 500–1,000 mcg | Water |
| Vitamin C | With iron-rich meals | 250–500mg | Food |
| Beta-alanine | 30–60 min pre-workout | 3.2g | Water |
| Citrulline Malate | 30 min pre-workout | 6–8g | Water |
Prices and supplement formulations are subject to change — verify with the manufacturer before purchasing.
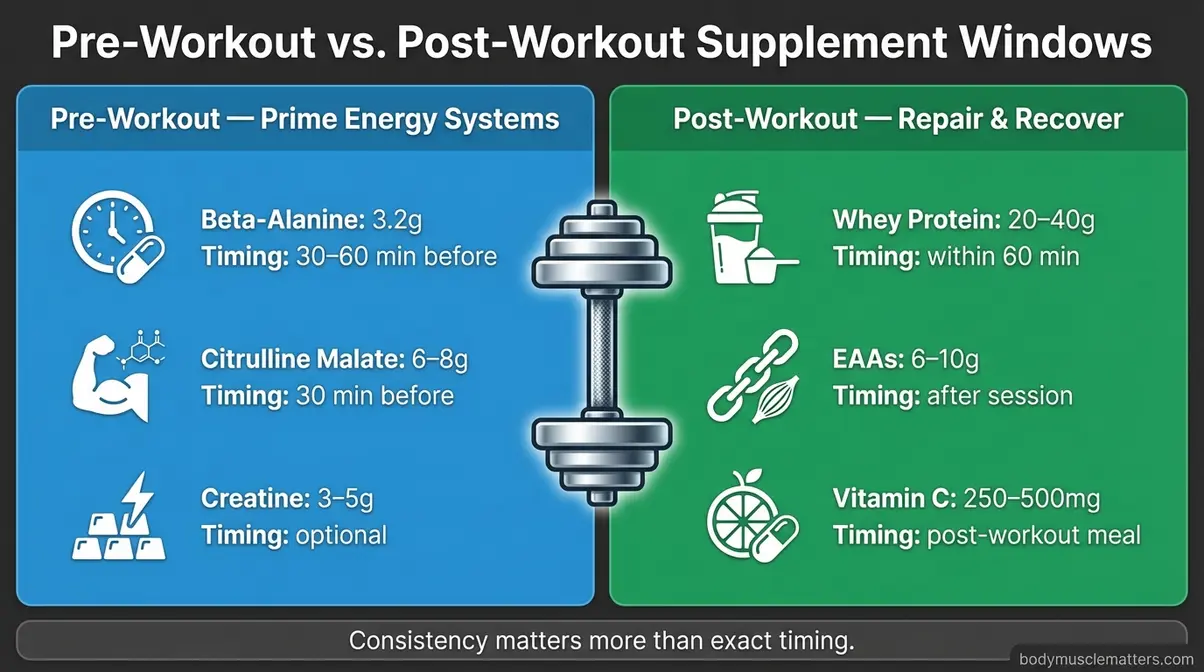
Caption: Pre-workout supplements (citrulline, beta-alanine, creatine) prime energy systems; post-workout supplements (whey, EAAs, Vitamin C) shift focus to repair and recovery.
Synergistic Pairs for Absorption
Certain supplements enhance each other when taken together. Others actively compete for absorption. Knowing the difference protects your investment.
- Synergistic pairs (take together):
- Vitamin D3 + Magnesium: Magnesium is required to convert Vitamin D into its active form. Without magnesium, Vitamin D supplementation is less effective — this pairing is foundational to the Foundation-First Protocol.
- Vitamin C + Iron: Vitamin C increases non-heme iron absorption by up to 67% — particularly important for plant-based athletes.
- Creatine + Carbohydrates: Taking creatine alongside a carbohydrate source improves cellular uptake via insulin response. A post-workout shake with creatine + fruit works well.
- Calcium + Vitamin D3: Vitamin D is required for calcium absorption in the gut. Without adequate Vitamin D, much of your dietary or supplemental calcium passes through unused.
- Antagonistic pairs (separate by 2+ hours):
- Zinc + Iron: Compete for the same absorption transporter — taking them simultaneously reduces the uptake of both.
- Calcium + Iron: Calcium inhibits iron absorption. Take calcium supplements at meals that don’t include your primary iron source.
- High-dose Vitamin C or E + Training adaptation: As noted in Step 1, mega-doses of antioxidant vitamins taken immediately post-workout may blunt the oxidative signaling that drives muscle adaptation (NIH PMC, 2026). Moderate doses are fine; heroic doses are counterproductive.
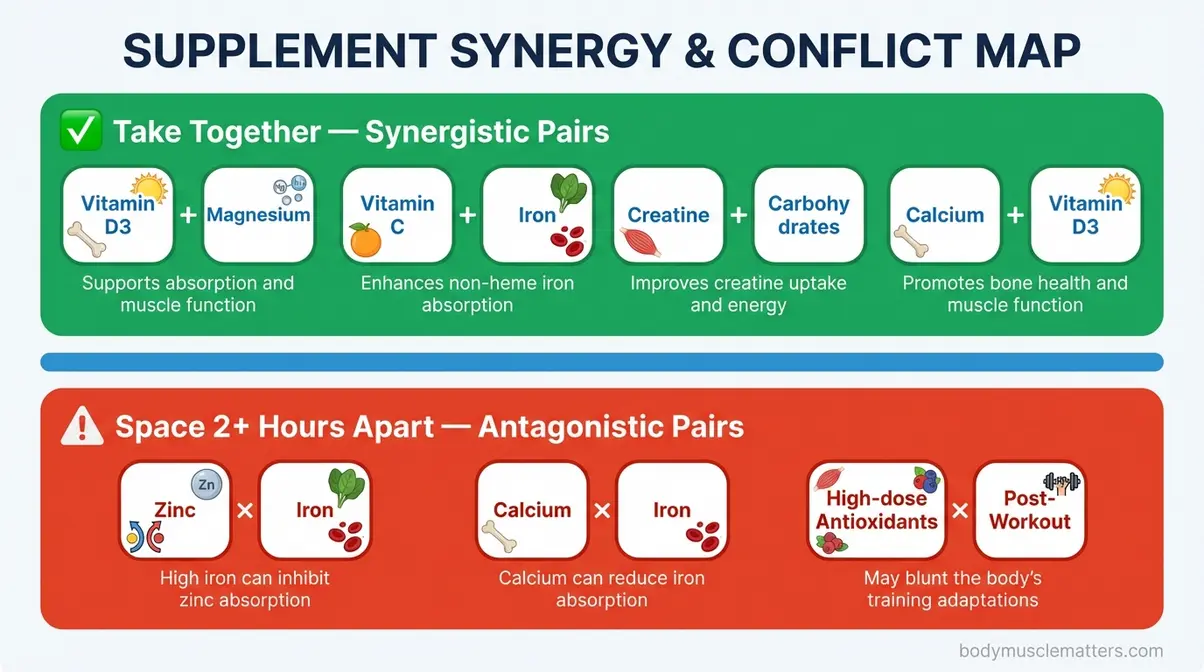
Caption: This synergy map shows which supplements to pair together and which to space 2+ hours apart — a simple rule set that meaningfully improves the efficiency of your full stack.
Common Mistakes and When to See a Doctor
Common Pitfalls Beginners Make
1. Skipping the foundation and starting with performance supplements. Taking creatine before addressing a Vitamin D or magnesium deficiency is the most common — and most expensive — mistake beginners make. The Foundation-First Protocol exists specifically to prevent this. Fix deficiencies first, then add performance supplements.
2. Taking too many supplements at once. Starting five new supplements simultaneously makes it impossible to identify what’s working or causing side effects. Introduce one supplement at a time, spaced 1–2 weeks apart. Track your training performance and note any changes.
3. Choosing low-quality mineral forms. Magnesium oxide, zinc oxide, and calcium carbonate are cheap forms with poor absorption. Look for glycinate, picolinate, and citrate forms instead. A supplement that isn’t absorbed isn’t doing its job — regardless of what the label claims.
4. Mega-dosing antioxidants. As noted throughout this guide, high-dose Vitamin C and E supplementation can blunt training adaptations (NIH PMC, 2026). Stick to recommended daily amounts through food and moderate supplementation.
5. Ignoring timing and pairing conflicts. Taking zinc with iron, or calcium with your iron supplement, reduces absorption of both. Follow the synergistic pairing table above — small adjustments in timing can meaningfully improve how much you actually absorb.
When to Consult a Doctor
Some situations require medical evaluation before, during, or instead of supplementation:
- Persistent fatigue and gym underperformance despite consistent training and adequate nutrition — get a blood panel checking ferritin, hemoglobin, B12, and Vitamin D levels.
- Suspected anemia or iron deficiency — do not self-supplement iron without a confirmed diagnosis. Excess iron is toxic.
- Postmenopausal women considering calcium + Vitamin D — some cardiovascular risk considerations exist at high calcium doses; discuss with your physician.
- Any existing kidney disease — creatine, high protein, and high-dose amino acids require medical clearance.
- Use of blood thinners or other medications — omega-3, Vitamin K, and several herbal supplements (including fenugreek) interact with anticoagulants.
- Symptoms that don’t resolve after 8–12 weeks of proper supplementation — consult a Registered Dietitian or sports medicine physician for a personalized assessment.
The right time to see a doctor is before you have a problem — not after. A basic blood panel costs less than one month of supplements and gives you far more actionable information.
Frequently Asked Questions
What vitamin is best for muscle growth?
Vitamin D3 is the single most important vitamin for muscle growth in most people. It directly signals muscle cells to increase protein synthesis, supports healthy testosterone levels, and regulates muscle fiber size. Research highlighted by Harvard Health Publishing confirms that Vitamin D deficiency is independently linked to measurable muscle strength loss across all age groups. A standard dose is 1,000–4,000 IU/day in D3 form. Most people who train indoors or live in northern climates are deficient and don’t know it, making supplementation a high-priority baseline step.
How can you grow muscle faster?
To grow muscle faster, combine three elements: resolve foundational deficiencies, optimize your stack, and match protein intake to training volume. First, follow the Foundation-First Protocol to address Vitamin D, Iron, and Magnesium deficiencies. Second, build your performance layer with creatine (3–5g/day) and whey protein isolate. Finally, progressive overload in training remains the primary non-negotiable driver of faster muscle growth.
What are the Big 3 supplements?
The Big 3 supplements for muscle growth are Creatine Monohydrate, Whey Protein Isolate, and Vitamin D3 — the combination with the strongest collective evidence base for building lean muscle. Creatine increases training volume capacity while whey protein delivers the leucine needed to maximally trigger muscle protein synthesis. Vitamin D3 regulates the intracellular signaling that makes protein synthesis possible in the first place.
Prices and supplement formulations are subject to change — verify with the manufacturer before purchasing.
The Foundation Determines Everything
For fitness beginners and intermediate gym-goers, the best vitamins for muscle growth work only when the micronutrient foundation is intact. A 2026 PMC network meta-analysis confirmed that collagen and whey are the only protein supplements that significantly enhance strength training effects — yet none of that matters if your Vitamin D, Iron, and Magnesium levels are depleted (PMC, 2026). The Foundation-First Protocol exists because fixing foundational deficiencies is the highest-leverage action available to anyone who’s training consistently but not progressing as expected.
The Foundation-First Protocol provides the sequencing that most supplement guides miss entirely. Address Vitamin D, Iron, and Magnesium first. Layer creatine and whey protein second. Customize for your gender, age, and hormonal status third. The protocol connects your initial frustration — spending money on supplements that don’t seem to work — to the real cause: a foundational gap that silently undercuts every product in your stack.
Your next step is concrete: get a basic blood panel this week. Test ferritin, hemoglobin, serum Vitamin D (25-OH), and B12. Then start at Step 1 of this guide and build from the bottom up. Choose one supplement at a time, spaced 1–2 weeks apart, so you can identify exactly what’s working. Most people who follow the Foundation-First Protocol see measurable improvements in training energy and recovery within 4–8 weeks of correcting confirmed deficiencies — before ever touching creatine or protein powder.
Related posts:
Best Protein Powder for Muscle Growth: Tested (2026)
Best High Protein Meal Delivery Services 2026: Top 7
Protein Powder Without Artificial Sweeteners: 10 Best Picks
Can You Eat Too Much Protein? Symptoms & Safe Limits
Best Protein Powder for Weight Loss: 10 Expert Picks
What Are Macros? A Plain Guide to Protein, Carbs and Fat
Callum
Hi, I'm Callum, the founder of Body Muscle Matters. I'm not a certified trainer, I'm a self taught lifter who started this site to share what I've learned from my own training and a lot of trial and error. Everything here comes from real experience and honest research, written the way I'd explain it to a friend who is just getting started. My goal is simple: practical, no hype fitness advice you can actually use.