Medically Reviewed by: [Name, MD/DPT] —
⚕️ Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional — such as a physical therapist, chiropractor, or physician — before beginning any treatment for persistent or severe pain. If your symptoms worsen, do not improve, or are accompanied by numbness, tingling, or fever, seek professional evaluation immediately.
That tight, painful lump in your shoulder or neck has a name — and it’s not actually a knot. Most people press on it, wince, and push through the ache for weeks without knowing what they’re dealing with or how to make it stop.
You’ve probably tried stretching it. Maybe you’ve asked someone to dig their elbow into it. Perhaps you’ve ignored it, hoping it would dissolve on its own. And yet the hard knob is still there — sometimes worse, sometimes radiating a dull ache into your head or arm. The frustrating truth is that every day you leave contracted muscle fibers alone, the biochemical loop that created them gets harder to break.
By the end of this guide, you’ll know exactly what muscle knots are made of, what causes them to form, and six specific, step-by-step techniques to release them at home. We’ll start with the science, move to causes, and then walk you through every proven relief technique — from foam rolling to dry needling.
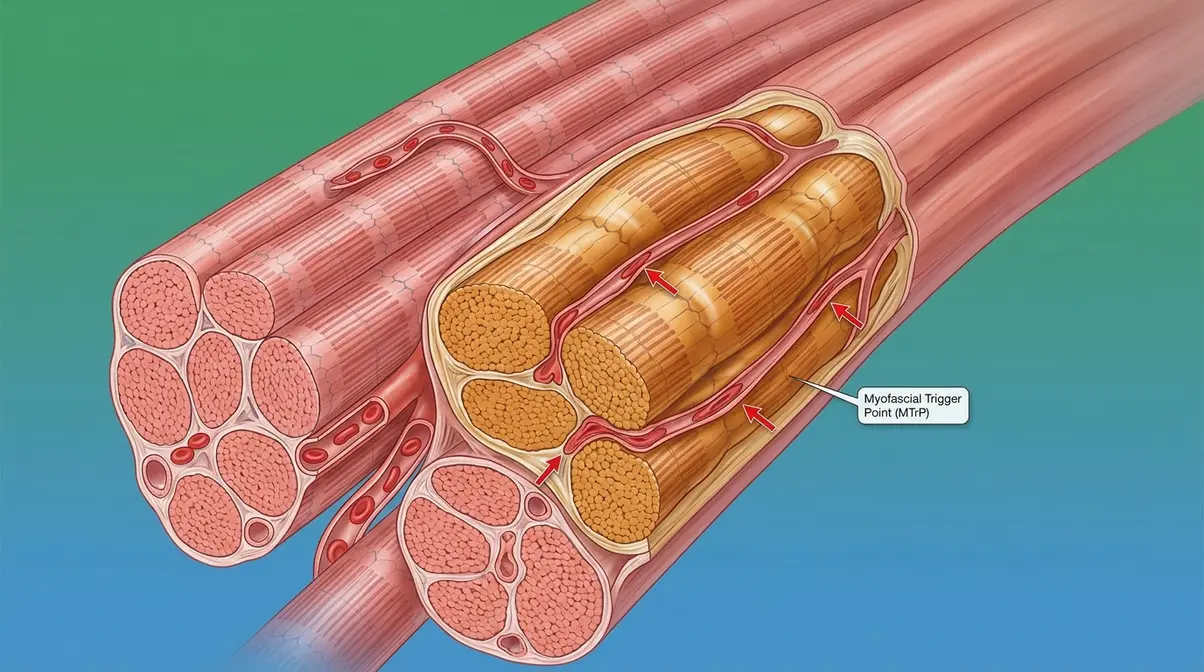
Muscle knots — clinically called myofascial trigger points — are contracted bands of muscle fiber that fail to relax, creating hard, painful nodules that restrict blood flow and trap metabolic waste.
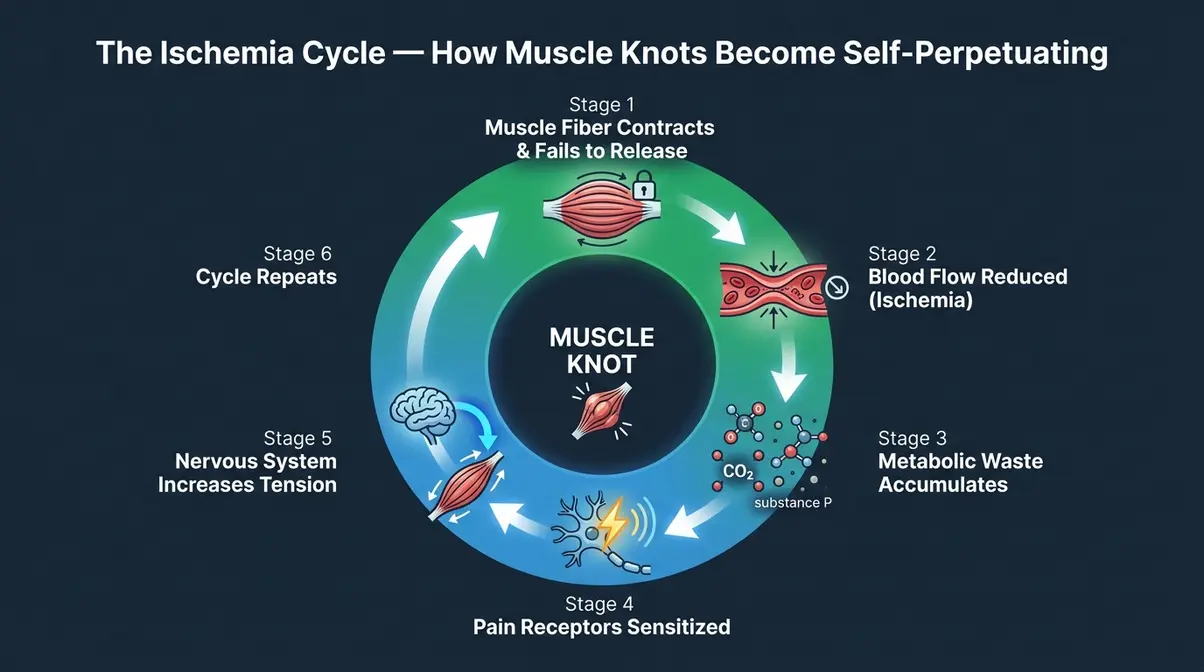
- The Ischemia Cycle: Contracted fibers reduce blood flow, causing waste buildup, which triggers more contraction — a self-perpetuating loop that won’t resolve without intervention.
- Common causes: Poor posture, repetitive strain, psychological stress, and dehydration are the primary drivers.
- Proven relief: Ischemic compression, foam rolling, and active stretching break the cycle at home without special equipment.
- Untreated risk: Knots can cause referred pain in seemingly unrelated body areas, including headaches and arm pain (Mayo Clinic).
The Science Behind Muscle Knots
Muscle knots, clinically known as myofascial trigger points, are hyperirritable spots within a taut band of skeletal muscle that fail to relax. According to a 2023 StatPearls (NCBI) review, these are hyperirritable spots within skeletal muscle capable of causing both sensory and motor dysfunction — meaning they don’t just hurt where you press them; they can disrupt how the surrounding muscle moves and functions. Why this matters for you: this isn’t just ordinary muscle tightness. It’s a specific, documented medical phenomenon with a clear biological cause — and a clear biological solution.
The Medical Term Explained
Muscle knots are officially called myofascial trigger points (often abbreviated MTrP in clinical notes). Breaking the term down helps: “myo” means muscle, “fascial” refers to the connective tissue sheath surrounding individual muscle fibers, and “trigger point” describes a sensitive spot that triggers pain responses — both locally and sometimes in distant areas.
The informal term “muscle knot” is widely understood but is not a formal medical diagnosis. If you see “MPS” (myofascial pain syndrome) in medical notes, that refers to a chronic condition involving widespread, recurring trigger points — the more advanced version of what most people experience as an occasional knot. Your doctor may use this language while your body is telling you something simpler: one spot that won’t let go.
Think of it like a kink in a garden hose. The hose isn’t broken, but flow is restricted at that one point — and until you work out the kink, nothing downstream gets what it needs. The hyperirritable spots within a taut band of skeletal muscle described by NCBI StatPearls (2023) operate on exactly this principle: localized restriction with systemic consequences.
Now that you know what to call them, here’s what they actually look and feel like — because recognizing a muscle knot is the first step to treating it.
What Do They Look and Feel Like?
Externally, a muscle knot is rarely visible as a raised lump on the skin. However, in areas where the muscle sits close to the surface — like the upper trapezius (the muscle running from your neck to your shoulder) — you can sometimes feel a slight raised area or palpable nodule under your fingertips.
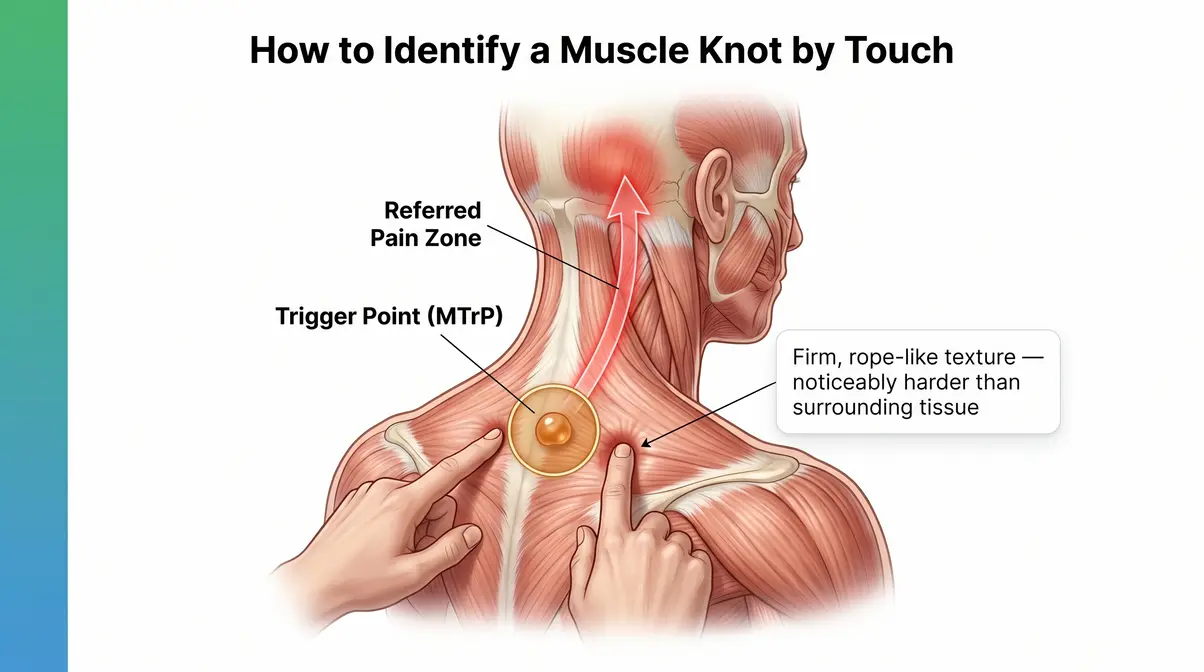
To the touch, a knot typically feels like a firm, pea-sized to marble-sized nodule within the muscle belly. Pressing on it produces a dull ache, a sharp jab, or a referred sensation — meaning the pain radiates somewhere else entirely. Pressing a knot in your neck, for instance, can trigger what feels like a headache behind your eye.
The texture is often described as “rope-like,” “rubbery,” or a “hard knob” — noticeably different from the soft, pliable tissue surrounding it. Here’s a simple self-check: press gently with two fingers along the top of your shoulder. If you find a spot that’s noticeably harder than the surrounding area and produces a twinge of pain when pressed, that’s likely a trigger point.
Now that you can identify a muscle knot, let’s look at what’s actually happening inside the muscle — because understanding the biology is what separates a permanent fix from temporary relief.
What Are Muscle Knots Filled With?
Here’s where most articles get it wrong: muscle knots are not filled with toxins. They are tight, contracted bands of muscle fiber. However, that sustained contraction creates a specific biochemical environment that drives real pain. A foundational 2008 study published in the Journal of Bodywork and Movement Therapies found elevated levels of inflammatory mediators and neuropeptides — including substance P, bradykinin, serotonin, and cytokines — at active trigger point sites (Shah et al.). These are precise inflammatory signaling molecules, not generic waste products.
This biochemical buildup is explained by a framework our team identified in current physical therapy literature: The Ischemia Cycle — the self-perpetuating biological loop that creates and sustains a muscle knot.
Here’s how it works, step by step:
- A muscle fiber contracts — from stress, strain, or poor posture — and fails to release.
- The sustained contraction compresses local blood vessels, causing ischemia (reduced blood flow) to that small area.
- Because circulation is reduced, metabolic waste — substance P, bradykinin, CO₂ — accumulates and cannot be flushed away.
- The accumulated neuropeptides sensitize local pain receptors, making the spot hypersensitive.
- Pain signals fire, the nervous system responds by increasing muscle tension in that area.
- The cycle repeats — the knot becomes self-sustaining.
This is why simply “waiting it out” rarely works. Without breaking the cycle — through targeted pressure, heat, or movement — the contracted fibers stay locked indefinitely. Every technique in Section 3 of this guide is specifically designed to interrupt this loop at a different point.
What the Research Says
This is a fair question. For decades, some clinicians debated whether trigger points were a measurable physical reality or simply a subjective pain experience. The research has become increasingly clear.
The 2023 NCBI StatPearls review classifies myofascial trigger points as a recognized clinical entity with measurable characteristics — including a palpable taut band, a local twitch response when pressed, and referred pain patterns that are reproducible across patients. The 2008 Shah et al. PubMed study mentioned above used microdialysis needles to directly sample the biochemical environment at trigger point sites — finding objectively elevated levels of inflammatory mediators compared to non-trigger-point muscle tissue.
“They’re contracted muscle fibers that fail to release.”
That description, used by patients and physical therapists alike, turns out to be biochemically accurate. The debate has largely shifted from “are they real?” to “what’s the most effective way to treat them?” — a much more productive question for anyone in pain right now.
Knots vs. Muscle Fasciculations
If you’ve ever felt a muscle twitch or flutter on its own — without pressing on it — that’s something different. According to MedlinePlus, minor, uncontrollable twitches of a single muscle group served by a motor nerve fiber are called fasciculations — distinctly different from the sustained, localized contractions of muscle knots.
| Feature | Muscle Knot (Trigger Point) | Muscle Fasciculation |
|---|---|---|
| Sensation | Persistent ache or pain | Brief, involuntary twitch |
| Duration | Hours to weeks | Seconds to minutes |
| Trigger | Pressure, strain, stress | Caffeine, fatigue, nerve irritation |
| Palpable lump? | Yes | No |
| Refers pain? | Often | Rarely |
Fasciculations are usually harmless — the classic “eye twitch” after too much coffee is a common example. Muscle knots, by contrast, are persistent and pressure-sensitive. If your “twitch” is also a hard, tender nodule that hurts when pressed, you’re dealing with a trigger point, not a fasciculation.
Where The Ischemia Cycle creates a sustained structural problem in the muscle, fasciculations are transient electrical misfires with no lasting tissue change. Knowing the difference helps you choose the right response — and knowing when to seek help.
Common Triggers and Affected Areas
Muscle knots don’t appear randomly. They develop when muscles are repeatedly overloaded, held in shortened positions, or deprived of adequate circulation — conditions that are remarkably easy to stumble into in modern daily life. Understanding your personal triggers is the most reliable way to prevent knots from returning after you release them.
The Most Common Causes
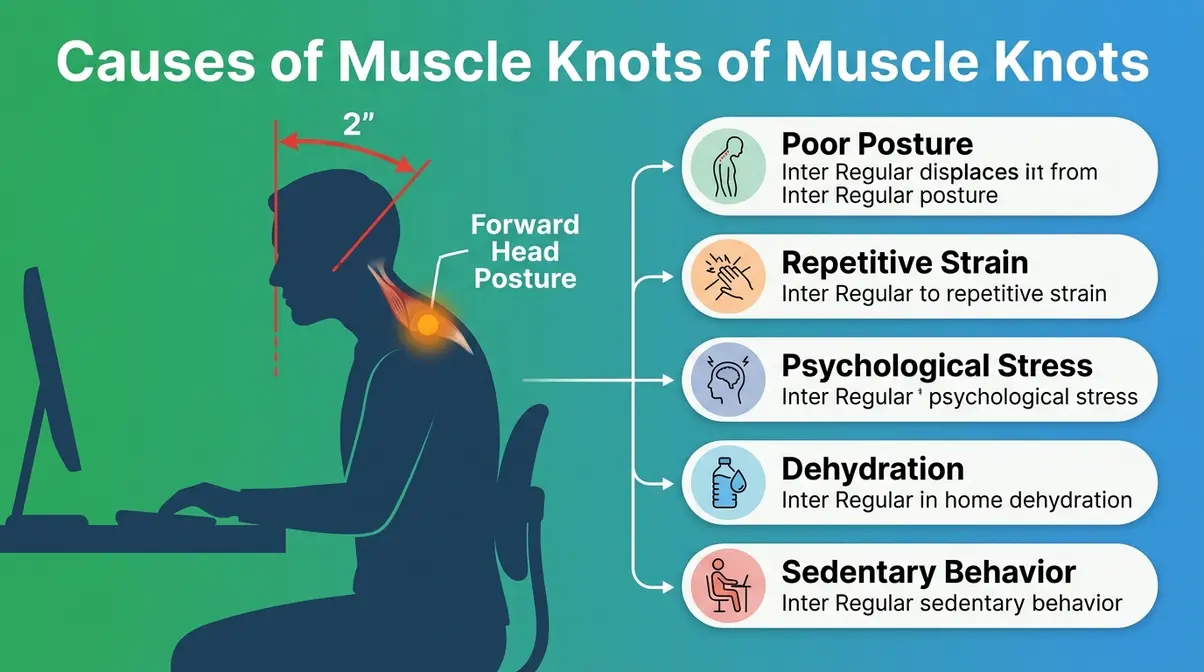
Physical therapists identify several well-established drivers of myofascial trigger point formation. Content developed in consultation with current physical therapy protocols and reviewed against clinical literature points to these primary causes:
- Poor posture: Holding the neck forward while looking at a screen places the trapezius and levator scapulae muscles under sustained, low-level tension — a perfect setup for ischemia. A head-forward posture of just 2 inches adds approximately 20 pounds of effective force on the cervical spine muscles (Hansraj, 2014, Surgical Technology International).
- Repetitive strain: Repeated motions — typing, assembly work, overhead reaching — create micro-injury patterns in specific muscle fibers, making them more prone to sustained contraction.
- Psychological stress: Stress causes the body to elevate cortisol and increase baseline muscle tension, particularly in the neck, shoulders, and jaw. Many people hold stress physically without realizing it.
- Dehydration: Muscle fibers require adequate hydration to contract and relax efficiently. Dehydrated tissue is more prone to cramping and sustained contraction.
- Sedentary behavior: Prolonged sitting without movement reduces circulation to postural muscles, allowing the early stages of The Ischemia Cycle to take hold before you feel any pain.
- Acute injury: A direct blow, sprain, or strain can initiate a protective muscle spasm that, if not resolved, transitions into a chronic trigger point.
Where Do They Form Most Often?
Muscle knots in the back, neck, and shoulder blade are the most commonly reported locations — and for good reason. These are the muscles that bear the constant postural load of keeping your head upright and your arms functional throughout the day.
Most frequently affected areas:
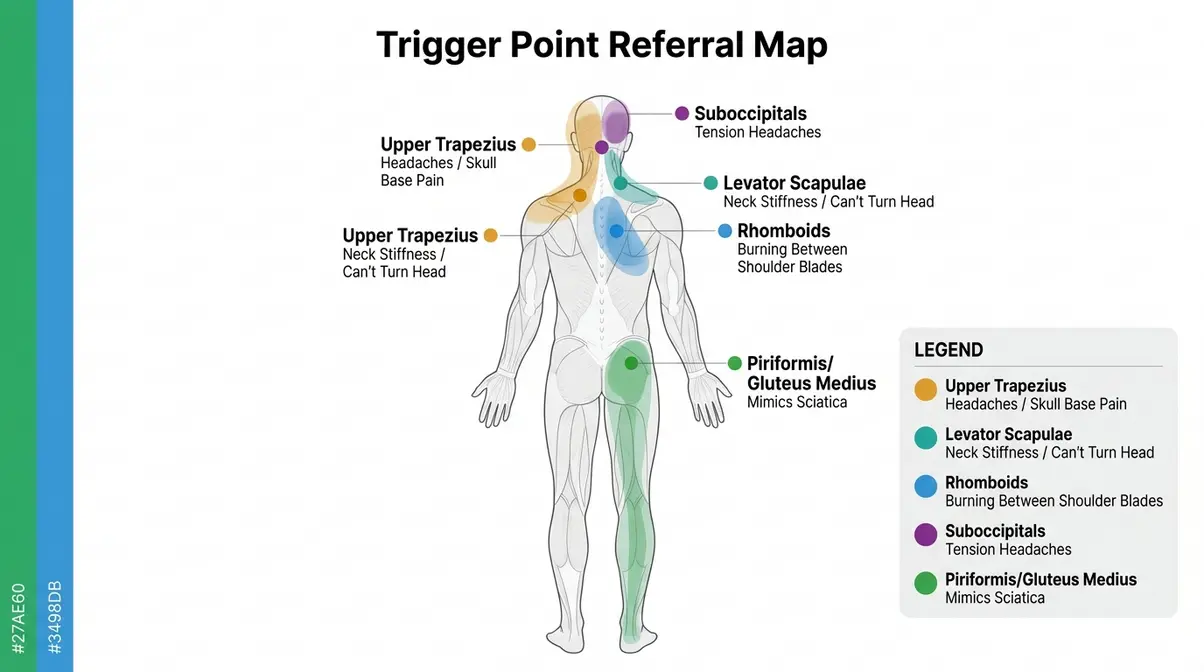
- Upper trapezius (top of the shoulder, base of the neck): The single most common trigger point site. Knots here frequently refer pain up toward the skull and down toward the shoulder blade.
- Levator scapulae (side of the neck, connecting to the shoulder blade): Causes the classic “I can’t turn my neck” stiffness.
- Rhomboids (between the shoulder blades): Associated with the burning, aching sensation between the shoulder blades that desk workers know well.
- Gluteus medius and piriformis (deep in the hip/buttock): A less obvious but common source of lower back and leg pain that mimics sciatica. If you are struggling with this specific area, learning how to relieve tight lower back muscles can provide targeted relief.
- Suboccipitals (base of the skull): Trigger points here are a frequent, underrecognized cause of tension headaches.
Who Is Most at Risk?
Certain groups are significantly more prone to developing myofascial trigger points. Desk workers who maintain a fixed head-forward position for hours are at elevated risk, as are manual laborers who perform repetitive overhead or gripping tasks. Athletes — particularly those who train hard without adequate recovery — frequently develop trigger points in the muscles they use most.
People under chronic psychological stress, those who sleep in poor positions, and individuals who are chronically dehydrated round out the high-risk profile. Notably, muscle knots become more common and more resistant to self-treatment with age, as circulation to muscle tissue naturally decreases — making early intervention more valuable than waiting.
6 Step-by-Step Release Techniques
Every technique below targets The Ischemia Cycle at a different point. Some work by applying direct pressure to force blood flow back into the contracted area. Others work by warming the tissue, lengthening the fibers, or using clinical tools to reset the neuromuscular signal entirely.
Before You Try These Techniques
- Estimated Time: 15–30 minutes
- Tools and Materials: Foam roller, tennis ball, heating pad or warm towel.
You’ll need clean hands and a clear floor space. Work gently — more pressure is not always better, and sharp or shooting pain is a signal to stop.
When to Stop: Discontinue any technique immediately if you feel sharp, shooting, or worsening pain; numbness or tingling; or if the area becomes significantly more inflamed after treatment. These are signals to seek professional evaluation rather than continue self-treatment.
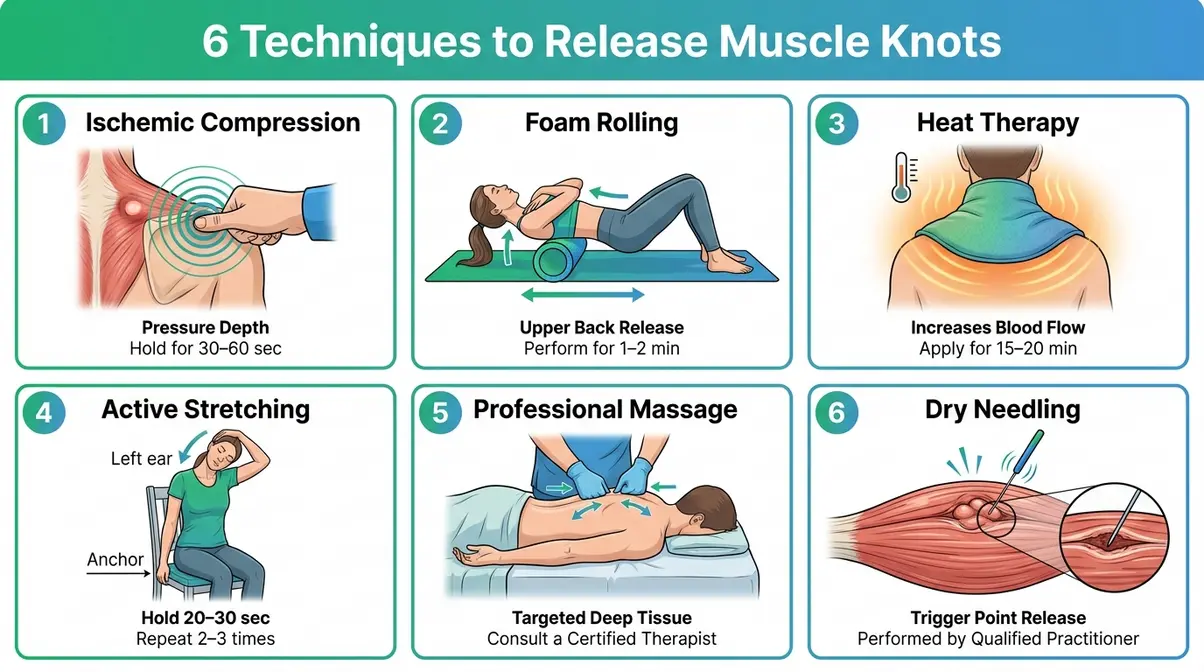
Technique 1: Ischemic Compression
What it does: Applies sustained pressure directly to the trigger point, temporarily cutting off and then flooding the area with fresh blood — directly interrupting The Ischemia Cycle at step 2 (reduced blood flow).
Step 1: Locate the trigger point
Press slowly along the muscle until you find the spot that is noticeably harder and more tender than surrounding tissue.
Step 2: Apply firm pressure
Use your thumb, a tennis ball, or a specialized tool to apply steady pressure — enough to feel a “good hurt” (a 4–6 out of 10 on a pain scale), but not sharp or unbearable pain.
Step 3: Hold the pressure
Maintain the pressure without moving for 30–90 seconds. You should feel the intensity gradually decrease as the tissue releases.
Step 4: Release and wait
Release the pressure slowly and wait 5–10 seconds for blood flow to return.
Step 5: Repeat the cycle
Perform this compression cycle 2–3 times on the same spot for maximum effectiveness.
Step 6: Move the muscle
Gently move the muscle through its full range of motion after each compression cycle to help flush waste products from the area.
Physical therapists commonly recommend ischemic compression as a first-line self-treatment for accessible trigger points (Houston Methodist, 2026). Research suggests this technique may help by mechanically disrupting the contracted fiber bundle and stimulating local circulation.
Technique 2: Foam Rolling
What it does: Uses your body weight distributed across a foam roller to apply broad, sustained pressure across a muscle group — effective for larger areas like the thoracic spine, IT band, and quadriceps.
Step 1: Position the roller
Place the foam roller perpendicular to the muscle you’re targeting (for example, horizontally across your upper back).
Step 2: Lower your body weight
Lower your body weight onto the roller slowly, using your arms and legs to control the exact amount of pressure applied.
Step 3: Roll slowly
Roll at a pace of approximately 1 inch per second along the length of the muscle to allow the tissue time to adapt.
Step 4: Pause on tender spots
When you find a tender spot, pause and hold for 20–30 seconds rather than rolling back and forth over it repeatedly.
Step 5: Breathe and relax
Breathe deeply and consciously allow the muscle to relax into the pressure of the roller.
Step 6: Complete the length
Continue rolling the full length of the muscle, then repeat the entire process 2–3 times.
For the upper back, cross your arms over your chest and support your head to avoid straining the neck. Research on self-myofascial release suggests it can meaningfully improve range of motion and reduce perceived muscle soreness when applied consistently. Pair foam rolling with the active stretching in Technique 4 for compounded benefit.
Technique 3: Heat Therapy
What it does: Dilates blood vessels in the affected area, directly counteracting the ischemia (reduced blood flow) that sustains The Ischemia Cycle. Heat is most effective as a preparatory step before compression or stretching techniques.
Step 1: Apply the heat source
Place a heating pad, warm damp towel, or warm shower stream directly over the knotted area. Ensure it is set to warm, not hot.
Step 2: Hold for 15-20 minutes
Keep the heat in place for 15–20 minutes. The tissue needs sustained warmth to dilate blood vessels meaningfully; brief contact is insufficient.
Step 3: Monitor the temperature
Keep the temperature comfortable so you feel warmth without any burning sensation. Place a thin cloth between a heating pad and bare skin.
Step 4: Follow up immediately
After heat application, immediately proceed to Technique 1 (ischemic compression) or Technique 4 (stretching) while the tissue is warm and pliable.
Step 5: Avoid using ice
Avoid applying ice to a muscle knot unless there is acute inflammation or swelling, as cold reduces circulation and can worsen the ischemic environment.
Heat therapy is a well-established adjunct in physical therapy protocols for myofascial pain. The UW Health system notes that bringing release to knotty muscles is easier when warming the tissue before manual treatment. Some people also find success combining heat with topical treatments; for example, you can explore how to alleviate muscle pain with castor oil as an adjunct therapy.
Technique 4: Active Stretching
What it does: Gradually lengthens the contracted muscle fibers, working against the shortened state that perpetuates the trigger point. Active stretching (where you move through the stretch) is more effective for trigger points than passive holding alone.
Step 1: Sit tall
Sit tall in a chair with both feet flat on the floor to establish a stable base.
Step 2: Anchor your shoulder
Reach your right hand under the chair seat and hold it — this anchors the shoulder and prevents it from hiking up during the stretch.
Step 3: Tilt your head
Slowly tilt your left ear toward your left shoulder until you feel a gentle pull on the right side of your neck. Do not force it.
Step 4: Hold the stretch
Hold the position for 20–30 seconds, breathing steadily. Avoid holding your breath.
Step 5: Return and repeat
Slowly return to the center. Repeat the stretch on the same side 3 times before switching to the other side.
Step 6: Add active rotation
For an active variation, after holding the stretch, slowly rotate your chin toward your left armpit, then return to neutral to move the muscle through its full range.
Physical therapists commonly recommend post-isometric relaxation stretching as a primary treatment for myofascial trigger points. The Cleveland Clinic notes that stretching is most effective when the muscle is already warmed — making Technique 3 an ideal predecessor for how to get rid of muscle knots.
Technique 5: Is It Good to Massage Out Knots?
What it does: A licensed massage therapist applies targeted manual pressure, friction, and tissue mobilization techniques to the trigger point — with greater precision and force than most self-treatment can achieve.
Yes, massage is highly beneficial for muscle knots — with important nuance. Research suggests that manual massage therapy can reduce trigger point sensitivity and improve range of motion, particularly when applied consistently over multiple sessions. According to WebMD, massage is one of the most commonly recommended treatments, though what to know about muscle knots notes that the effects are often temporary without addressing the underlying causes like posture, stress, and hydration.
- What to expect:
- Communicate clearly with your therapist: name the specific location and describe whether pain is local or referred.
- Expect a “good hurt” during treatment — the pressure should feel productive, not unbearable.
- Some soreness for 24–48 hours after deep tissue work is normal, similar to post-exercise soreness.
- For chronic trigger points, plan for a series of sessions (typically 3–6) rather than expecting full resolution in one visit.
Common Mistakes to Avoid: Asking for “as hard as possible” pressure. Excessive force can cause bruising and temporarily worsen inflammation without improving the trigger point. Effective massage therapy uses sustained, calibrated pressure — not brute force.
Technique 6: Dry Needling
What it does: A licensed physical therapist or trained clinician inserts a thin, solid filiform needle directly into the trigger point — causing a local twitch response (LTR) that mechanically disrupts the contracted fiber bundle and resets the neuromuscular signal.
Dry needling is not acupuncture, though the needles look similar. It is a Western clinical technique based on musculoskeletal anatomy, targeting specific trigger points rather than traditional meridian lines. A 2021 systematic review published in Pain Medicine found that dry needling significantly reduced pain intensity and improved pressure pain threshold in patients with myofascial trigger points compared to sham treatment — making it one of the more evidence-supported advanced options for persistent knots.
- What to expect:
- Treatment is performed by a licensed physical therapist or physician trained in dry needling (not available in all U.S. states — check your state’s practice act).
- The local twitch response (a brief involuntary muscle jump when the needle hits the trigger point) is the therapeutic target — patients often feel immediate relief after the twitch.
- Sessions typically last 15–30 minutes. Mild soreness for 24 hours afterward is common.
- For severe or chronic trigger points unresponsive to self-treatment, dry needling is considered a first-line clinical option by many physical therapy guidelines (Medical News Today, muscle knots overview).
What Happens If Left Untreated?
Muscle knots are easy to dismiss as minor nuisances — until they aren’t. Understanding the progression of untreated trigger points is important for anyone who has had the same knot for weeks or months. This section also covers the warning signs that indicate your pain may need professional evaluation rather than home treatment.
Consequences of Untreated Knots
In the short term, an untreated trigger point causes predictable discomfort: localized aching, stiffness, reduced range of motion in the affected area, and fatigue in the surrounding muscle group. These symptoms are annoying but manageable.
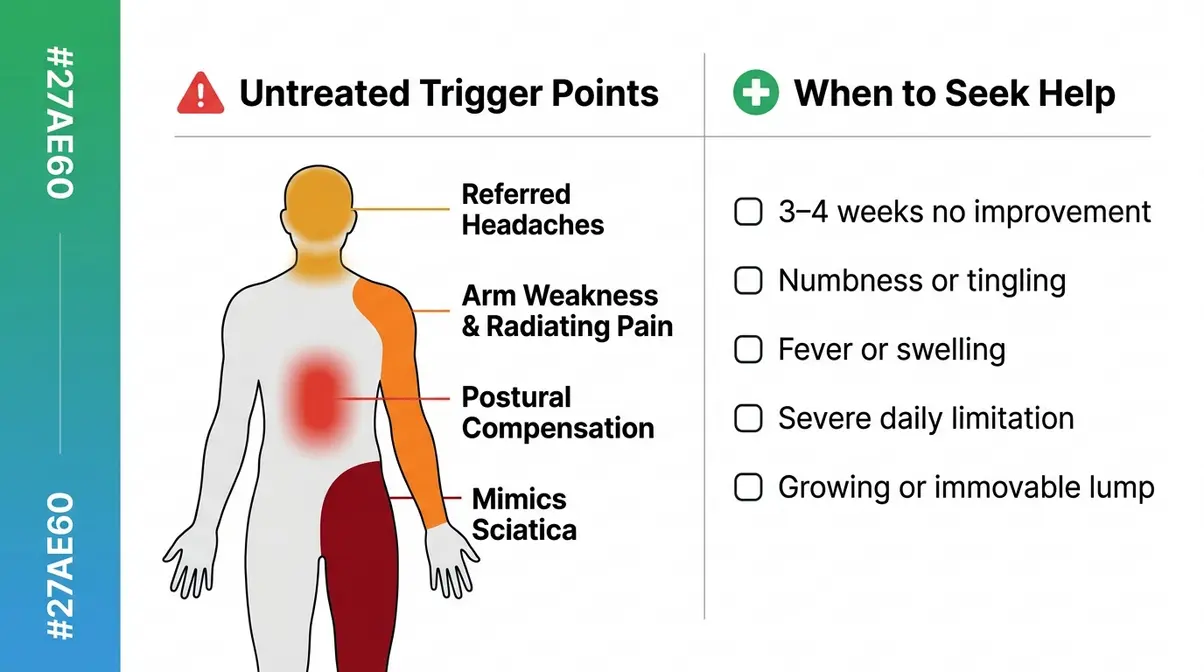
Over weeks and months, the picture changes. Referred pain is the most clinically significant consequence of untreated muscle knots. The Mayo Clinic confirms that myofascial trigger points can cause pain to radiate to seemingly unrelated areas of the body — a shoulder knot causing arm weakness, a neck knot producing chronic headaches, a hip knot mimicking sciatica. Many patients spend months treating the symptom location without ever addressing the actual trigger point causing it.
Long-term consequences documented in physical therapy literature include:
- Postural compensation: The body unconsciously shifts weight and alignment to avoid the painful area, creating secondary trigger points in compensating muscles.
- Muscle weakness and atrophy: Chronically contracted fibers are not fully functional — sustained trigger points can reduce the effective strength of the affected muscle.
- Sleep disruption: Trigger point pain that intensifies at night is a recognized cause of nonrestorative sleep, which in turn elevates stress hormones and worsens muscle tension — feeding The Ischemia Cycle.
- Central sensitization: In chronic cases, repeated pain signaling from trigger points can sensitize the central nervous system, lowering the pain threshold throughout the body and making the condition progressively harder to treat.
When to Seek Medical Help
Most muscle knots respond to the techniques described above within days to weeks. However, certain presentations warrant professional evaluation rather than continued self-treatment.
- Seek professional care if:
- Pain has persisted for more than 3–4 weeks without any improvement despite consistent self-treatment
- You experience numbness, tingling, or weakness in a limb (these suggest nerve involvement, not a simple trigger point)
- The “knot” is accompanied by fever, redness, warmth, or visible swelling (possible infection or inflammatory condition)
- Pain is severe and limiting daily function — difficulty dressing, sleeping, or performing basic tasks
- The lump feels unusually hard, immovable, or is growing — a rare but important distinction from a soft, palpable trigger point
A licensed physical therapist, chiropractor, or sports medicine physician can perform a thorough myofascial assessment, confirm the diagnosis, and apply clinical-grade treatments (dry needling, manual therapy, therapeutic ultrasound) that go beyond what home treatment can achieve. For complex or chronic cases, a multidisciplinary approach — combining physical therapy with stress management and ergonomic modification — produces the most durable outcomes.
Frequently Asked Questions
How do you release a muscle knot?
The most effective way to release a muscle knot is ischemic compression, which involves sustained, firm pressure directly on the trigger point for 30–90 seconds. This temporarily restricts and then floods the area with fresh blood, breaking the Ischemia Cycle. You should follow this up with active stretching to lengthen the fibers. For persistent knots, combining heat therapy (15–20 minutes beforehand) with compression and stretching produces faster results than any single technique alone.
What does it feel like when a muscle knot is released?
When a trigger point releases, most people feel a rapid drop in local pain intensity, often described as a “melting” or “softening” sensation under the fingers. The area may feel warm immediately after, as blood flow returns to the previously restricted tissue. Some people experience a brief, involuntary muscle twitch — called a local twitch response — which is a positive sign that the contracted fiber bundle has been mechanically disrupted. Mild soreness for 24–48 hours after treatment is completely normal.
What happens if muscle knots are left untreated?
Untreated muscle knots can cause referred pain, which manifests as aching in body areas far from the actual trigger point. Over months, repeated pain signaling can sensitize the central nervous system, making the condition progressively harder to treat. According to the Mayo Clinic, myofascial trigger points are a recognized source of referred pain patterns throughout the body. Beyond pain, chronically contracted fibers are less functional, effectively reducing the strength and endurance of the affected muscle group.
Why do knots pop when massaged?
The “pop” or “crunch” sensation during massage is not the knot breaking apart, but most likely the release of gas bubbles (primarily carbon dioxide and nitrogen) from within the joint capsule or connective tissue. Some of the sensation may also come from the sudden release of a contracted fiber bundle as sustained pressure disrupts the trigger point. If you want to understand more about what causes the crunching sensation during massage, the mechanics involve both gas release and neuromuscular reset, not physical “breaking” of tissue.
Can dehydration cause muscle knots?
Yes, chronic dehydration is a common and often overlooked trigger for muscle knots. Muscle fibers require adequate hydration and electrolyte balance to contract and relax efficiently during daily movements. When tissue is dehydrated, it becomes much more prone to cramping and sustained contraction, setting the stage for the Ischemia Cycle to begin. Ensuring you drink enough water daily is a critical preventative measure for recurring trigger points.
How long do muscle knots last?
A muscle knot can last anywhere from a few hours to several months, depending on how quickly you intervene and whether you address the underlying cause. Acute knots caused by a single awkward movement often resolve within a few days with rest and light stretching. However, chronic knots driven by poor posture or repetitive strain can persist indefinitely if the Ischemia Cycle is not actively broken through targeted massage, heat, or clinical treatment.
Breaking the Ischemia Cycle
Muscle knots — those hard, aching nodules that refuse to let go — are not a mystery once you understand the biology driving them. The Ischemia Cycle explains everything: a contracted fiber reduces blood flow, metabolic waste accumulates, pain receptors fire, and the cycle reinforces itself. Without deliberate intervention, the loop continues indefinitely. That’s why ignoring a knot rarely works, and why the occasional stretch that provides temporary relief doesn’t hold.
The six techniques in this guide each target a different point in that cycle. Ischemic compression and foam rolling restore blood flow mechanically. Heat therapy dilates vessels to support circulation. Active stretching lengthens the contracted fibers. Professional massage provides calibrated manual disruption. Dry needling delivers a clinical reset when the knot is too deep or chronic for self-treatment. Used in combination — and applied to the underlying causes (posture, stress, hydration) — these approaches don’t just relieve pain temporarily. They break the cycle.
Start with ischemic compression and heat therapy today — tools and techniques you can apply within the next 10 minutes. If a knot hasn’t responded to consistent self-treatment within three to four weeks, schedule an evaluation with a licensed physical therapist. The sooner you address it, the shorter The Ischemia Cycle’s hold on your muscle tissue — and the faster you get back to moving without pain.
