
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Consult your physician or a certified fitness professional before beginning any new exercise program, especially if you have a pre-existing health condition, are pregnant, or are postmenopausal.
Most women trying to lose weight or get fit default to the treadmill or cycling class. But a growing body of clinical research suggests that the weight room — not the cardio deck — is where the most transformative health changes happen.
Without resistance training (any exercise making your muscles work against a force, like dumbbells or bands), women naturally lose 3–8% of muscle mass per decade after age 30. That loss compounds — accelerating metabolic slowdown, weakening bones, and making everyday movements harder as the decades pass.
“Resistance training improves strength, body composition, bone health, cardiovascular function, mental health, self-esteem, and body image.”
In this 2026 guide, you will learn exactly why the benefits of resistance training for women make it the single most powerful health investment you can make — and how to begin safely. We cover the core physical benefits, bust the most persistent myths, address life-stage concerns (including menopause), and give you a clear beginner’s framework to get started. This guide draws on peer-reviewed clinical trials, NIH databases, and Tier 1 medical institutions including the CDC, NHS, and PubMed Central.
- Bone density: Weight-bearing resistance training signals bone-forming cells, slowing and reversing age-related bone loss at the hip, spine, and wrist
- Metabolism: Muscle tissue burns more calories at rest, making fat loss easier without chronic calorie restriction — and the EPOC effect keeps burning for up to 24 hours after your session
- Menopause: Strength training significantly reduces hot flashes, weight gain, and mood disruption during hormonal transitions (PMC, 2026)
- The Strength Dividend: Every consistent session compounds — the health returns from resistance training grow larger with each passing year, just as a financial investment multiplies over time
- Getting started: 2–3 sessions per week using the 3-3-3 rule is all beginners need to see real results within 10 weeks
Why Resistance Training Transforms Women’s Health

The benefits of resistance training for women extend far beyond aesthetics. Clinical research consistently links consistent weight training to stronger bones, a faster resting metabolism, improved cardiovascular health, and measurable reductions in anxiety and depression. A 2026 NHLBI analysis found that women may actually realize greater proportional health benefits from regular exercise than men — making the case for starting even more compelling (NHLBI, 2026). That means the benefits of weight lifting for women reach directly into longevity, mental resilience, and how confidently you move through daily life.
This section unpacks the biology — plainly, specifically, and with the clinical evidence behind each claim.
Resistance Training and Bone Strength
As the chart below illustrates, the gap between women who resistance train and those who do not widens significantly after menopause. Understanding why requires a brief look at bone biology — and the news is genuinely reassuring.
When you lift a weight or push against resistance, the force travels through your skeleton. That mechanical stress activates osteoblasts (bone-forming cells) — specialized cells that respond to physical loading by depositing new bone mineral. Think of it like heat stress on metal: just as controlled heat makes steel stronger, mechanical stress on bone makes it denser and more resistant to fracture. This process does not happen automatically with age — it requires a stimulus, and resistance training is among the most powerful stimuli available.
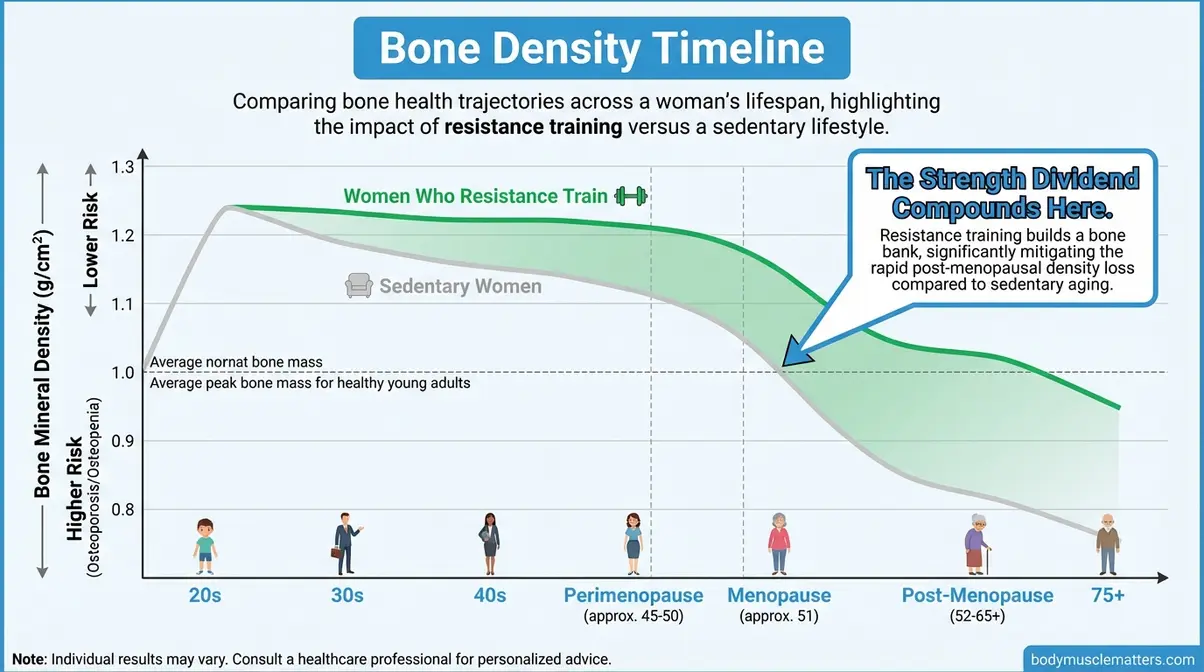
Caption: Bone mineral density in women who resistance train (blue) vs. sedentary women (grey) across life stages — the gap widens sharply after menopause, illustrating The Strength Dividend compounding over time.
The clinical evidence for this effect is landmark. The LIFTMOR — Lifting Intervention for Training Muscle and Osteoporosis Rehabilitation — trial, a landmark Australian clinical study led by Watson et al. (2018), compared high-intensity resistance and impact training against a standard low-intensity program in postmenopausal women with low bone mass. After eight months, the high-intensity group demonstrated statistically significant improvements in femoral neck bone mineral density compared to significant declines in the control group — a finding that challenged the long-held assumption that postmenopausal women should avoid high-load exercise (Watson et al., Journal of Bone and Mineral Research, 2018).
Resistance training activates osteoblasts — bone-forming cells — to build new bone mineral at the hip, spine, and wrist, the three sites most vulnerable to osteoporosis fractures (PMC, 2018).
It is also worth distinguishing resistance training from weight-bearing cardio like walking or jogging. Both benefit bone health, but resistance training generates stronger, more targeted mechanical forces at the specific fracture sites — the hip joint, lumbar spine, and wrist — that matter most. NIH research on resistance exercise and bone density confirms that power-type and high-intensity resistance training can be more effective than traditional lower-load protocols for improving and maintaining bone mineral density in postmenopausal women (PMC, 2018).
Consider a practical example: a 55-year-old woman performing two sessions of squats and deadlifts per week is actively stimulating the bone-forming process that would otherwise remain dormant in a sedentary lifestyle. Research suggests women can lose a significant portion of their bone density in the years following menopause — and resistance training is one of the only lifestyle interventions shown to reverse, not merely slow, this process (Mayo Clinic, 2026). For a deeper look at bone health after 50, see our guide on strength training’s impact on osteoporosis and hormones.
For a visual demonstration of safe bone-loading exercises, watch the expert walkthrough above.
Stronger bones are only the beginning — resistance training also fundamentally rewires your body’s ability to burn calories, even hours after you leave the gym.
The Metabolic Engine: Muscle Burns More
Here is a concept that surprises many beginners: your muscles burn calories even when you are doing absolutely nothing. Understanding why requires two plain-English definitions.
Resting metabolic rate (RMR) is the number of calories your body burns simply to keep you alive — breathing, pumping blood, maintaining body temperature. It accounts for 60–70% of your daily calorie burn. Muscle tissue is metabolically expensive — it requires significantly more energy to maintain than fat tissue does. Think of your muscles as a furnace: the bigger the furnace, the more fuel it burns even while idling. Adding even a modest amount of lean muscle through resistance training raises your RMR, which means you burn more calories around the clock — not just during exercise.
The metabolic benefits of resistance training for women are particularly relevant during the 30s, 40s, and 50s, when muscle loss quietly accelerates. But the second mechanism is what truly sets strength training apart from cardio.
EPOC — Excess Post-exercise Oxygen Consumption — is the calorie-burning effect that continues after your workout ends. After a strength training session, your body works to repair micro-damaged muscle fibers, restore oxygen balance, and return hormones to baseline. That recovery process requires energy. Research shows this elevated metabolism can persist for up to 24 hours following a resistance session, with some studies documenting measurable effects extending even longer (PMC, 2026). A 2026 PMC study comparing resistance training and high-intensity interval training found that resistance training maintained elevated resting metabolism for longer periods post-exercise.
The contrast with steady-state cardio is meaningful. A 30-minute run burns calories during those 30 minutes — then stops. A 30-minute strength session burns calories during the session AND continues burning for hours afterward through EPOC. PubMed meta-analysis on training frequency and strength confirms that training major muscle groups 2 to 5 days per week produces significantly superior metabolic adaptation compared to once-weekly training (PMC, 2019).
Muscle tissue is the body’s metabolic engine — and resistance training is the only reliable way to build and maintain it after age 30 — a distinction that separates strength training from every other form of exercise.
For a woman whose metabolism has felt sluggish since her 30s or 40s, muscle loss is the hidden driver. Resistance training addresses the root cause rather than just managing the symptom through diet restriction.
Beyond bones and metabolism, resistance training delivers a benefit that surprises most beginners: a significant reduction in heart disease risk — one of the top killers of women worldwide.
Your Heart Health Gets a Boost Too
The cardiovascular benefits of strength training for females are now well-documented in clinical literature — and they are more substantial than most women realize.
A large PMC meta-analysis found that women engaging in resistance exercise 1–3 times per week experienced a 55% reduction in total cardiovascular disease events compared to women who did no resistance training (PMC, 2020). A separate analysis of resistance training and mortality found a 21% lower all-cause mortality risk from resistance training alone — rising to a 40% reduction when combined with aerobic exercise (PubMed, 2019). These are not modest improvements; they represent one of the most compelling arguments for picking up a weight.
Regular resistance training is associated with a significantly reduced risk of cardiovascular-related death — one of the most underappreciated benefits of weight training for females (PMC, 2020).
The biological mechanisms are understandable in plain terms. Resistance training improves insulin sensitivity — how efficiently your cells respond to the hormone that manages blood sugar — which reduces the arterial inflammation that drives heart disease. It also lowers resting blood pressure over time and improves cholesterol profiles. None of these require you to become a competitive powerlifter; clinical benefits appear at frequencies as low as twice per week.
The honest answer on cardio vs. weights for heart health: both help, and the research is clear that combining resistance training with some aerobic activity produces the best cardiovascular outcomes. It is not an either/or choice. A woman doing two 30-minute resistance sessions per week plus two 20-minute brisk walks creates a cardiovascular stimulus comparable to — or exceeding — most gym cardio routines, based on current dose-response data.
The physical benefits of resistance training extend beyond the body — the most consistent, and often most surprising, impact women report is on their mental health.
Mental Health and Confidence
During and after a resistance training session, your brain releases three key chemicals simultaneously: endorphins (natural mood elevators that create the well-known exercise “high”), serotonin (the brain chemical associated with calm and emotional stability), and dopamine (associated with focus, motivation, and reward). No pharmaceutical delivers all three at once, and few lifestyle interventions match the breadth of this neurochemical effect.
Research on the clinical implications is growing rapidly. A 2026 review in Trends in Molecular Medicine found that resistance exercise training produced small-to-moderate improvements in anxiety symptoms and significant reductions in depression symptoms — comparable to antidepressant medication and behavioral therapies in some populations, based on meta-analyses (Clinical Advisor, 2026). A 2026 PMC meta-analysis confirmed that resistance training produced greater improvements in depressive symptoms and self-esteem than other exercise modalities (PMC, 2026). Use appropriately qualified language here: research suggests resistance training can meaningfully reduce anxiety and depression symptoms — it does not replace clinical treatment.
Resistance training stimulates endorphin, serotonin, and dopamine release simultaneously — making it one of the most evidence-supported lifestyle interventions for women’s mental health.
Perhaps the most durable benefit is on self-esteem. As women grow stronger and discover physical capabilities they did not know they had, the psychological reference point shifts. The motivation evolves from “I want to look different” to “I can do things I could not do before.” Women who begin a 10-week beginner program frequently report feeling more confident in professional settings, more energetic in parenting roles, and less anxious overall — regardless of how their body composition changes. This capability-based confidence is documented repeatedly in body image research and reported consistently across community fitness forums.
These mental benefits compound with the final physical benefit of this section: the way resistance training rewires your body for everyday life.
Functional Strength for Daily Life
Functional strength — the ability to perform everyday physical tasks without strain or injury — is the everyday dividend that resistance training pays from your very first session. It is also, quietly, the benefit with the most dramatic quality-of-life implications.
Resistance training builds the specific muscle groups used in real-world movements: carrying grocery bags (biceps, core, upper back), climbing stairs (quadriceps, glutes), picking up children or grandchildren (lower back, core, legs), and getting up from a low chair or the floor (hip flexors, quads, abdominals). Women who squat and deadlift regularly find that these exact movements — the ones that feel hardest as women age without training — become noticeably easier within weeks.
Functional strength decline is one of the earliest indicators of aging, and one of the most preventable. Women who maintain it through their 50s and 60s have significantly lower rates of falls and fall-related fractures — a critical safety consideration given that hip fractures carry serious long-term health consequences in older adults. For a step-by-step breakdown of the exercises that build this foundation, see our comprehensive guide to developing functional strength.
Now that you understand the ‘why’ behind resistance training’s power, let us address the concern that stops most women from ever picking up a weight in the first place: the fear of getting bulky.
The Bulking Myth: Women Get Lean, Not Large

The number one reason women avoid the weights section is the fear of waking up one day looking like a bodybuilder. It is one of the most persistent myths in fitness — and it is completely at odds with female physiology. Here is the biological reality.
This is precisely why The Strength Dividend for women looks fundamentally different from men’s: you collect the metabolic, bone, and cardiovascular returns without the size returns. Hormones determine that outcome — and the hormonal difference between men and women is enormous.
The Hormonal Truth About Female Muscle
The fear of “bulking up” is understandable — and physiologically unfounded for the vast majority of women.
Testosterone is the primary anabolic hormone responsible for large-scale muscle growth. Men produce roughly 15–20 times more testosterone than women — a ratio confirmed by clinical endocrinology research (PubMed, 2001). If you picture men’s testosterone levels as a fire hose and women’s as a garden hose, the scale of the difference becomes intuitively clear. PubMed research on female testosterone response to exercise shows that the acute testosterone response to resistance exercise in women is minimal and transient — producing strength gains without causing significant muscle hypertrophy (the scientific term for major muscle size increase) or “bulking up” (PubMed, 2001).
Women produce 15 to 20 times less testosterone than men — making significant muscle bulk physiologically impossible without performance-enhancing substances (PubMed, 2001).
What women build through resistance training is something entirely different: definition, tone, and shape. Resistance training reshapes the body by increasing muscle fiber density and reducing body fat percentage — creating the sculpted appearance most women specifically want. The muscle fibers grow stronger and more defined, not dramatically larger.
The “toned arms” outcome most women are seeking IS precisely the result of resistance training — just not through the route they imagined. It comes from building lean muscle beneath the skin AND reducing the body fat layer covering it. For a full breakdown of the science behind female muscle growth, explore the truth about weightlifting and bulking up.
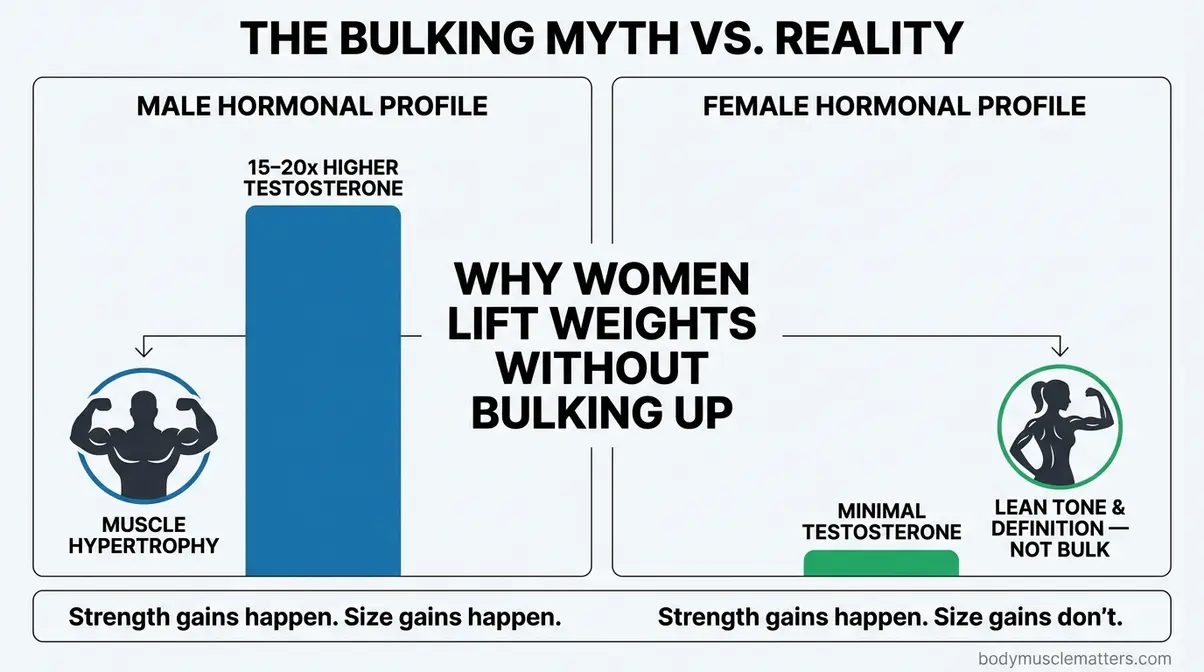
Caption: Female and male testosterone profiles at rest and post-exercise — the hormonal gap explains why women who lift become leaner and stronger, not larger.
Understanding the hormonal reality resolves the bulking fear — but it raises a natural follow-up question: if not weights, should I just do more cardio for fat loss? The research has a clear answer.
Weights vs. Cardio: What Research Shows
Cardio burns calories during the session and stops. Resistance training burns calories during AND after — as discussed in the metabolic section, the EPOC mechanism keeps your metabolism elevated for up to 24 hours post-workout. This is not a minor distinction for women managing weight without extreme calorie restriction.
For body composition — the ratio of fat to muscle — research consistently shows resistance training outperforms steady-state cardio when calorie intake is matched. The reason is straightforward: sustained cardio at high volumes burns both fat AND muscle tissue, particularly the fast-twitch fibers that drive strength and power. Resistance training, by contrast, preserves and builds muscle while promoting fat loss. Cardio at high volumes can erode muscle maintenance — the very tissue responsible for your long-term metabolic rate.
The practical implication: two 45-minute strength sessions per week consistently outperform five 30-minute treadmill sessions for long-term fat loss in women — because muscle gained burns fat passively, 24 hours a day.
For women prioritizing body composition, resistance training delivers superior fat-loss outcomes compared to cardio alone — because the muscle built continues burning calories long after the session ends.
The optimal approach for most women with limited time is resistance-first, with incidental walking or light cardio on recovery days. The research does not frame this as a competition — it frames it as a priority question. And for body composition and metabolic health, resistance training earns the top spot.
The practical result of that fat-burning, muscle-building process is not a bulky physique — it is the lean, defined appearance that most women are actually seeking.
Building the Lean, Toned Look You Want
If flabby arms or soft thighs are your specific concern, resistance training is the most direct answer science provides. The “toned” aesthetic comes from two processes happening simultaneously: building the muscle underneath, and reducing the fat on top. Cardio alone accomplishes only the second — which is why many women who run or cycle exclusively feel “soft” even when the scale moves.
Exercises like overhead tricep extensions, bicep curls, and resistance band rows directly target the arm and shoulder muscles that create the defined upper body look. Squats, hip thrusts, and Romanian deadlifts address the lower body. Both areas respond reliably to consistent resistance training, regardless of starting point.
And yes — toning arms after 50 is absolutely achievable. Muscle responds to resistance training at any age; the timeline may be slightly longer, but the process works. Research confirms that even adults in their 60s and 70s demonstrate meaningful muscle gains with progressive resistance training.
Resistance training is the most direct evidence-based solution for arms, legs, and core that feel soft — because it builds the muscle and burns the fat simultaneously, something cardio alone cannot do.
With the bulking myth firmly behind us, let us turn to the women who stand to gain the most from resistance training: those navigating the hormonal shifts of perimenopause, menopause, and the decades beyond.
Strength Training Through Every Stage of Life

Every year of consistent resistance training deposits into your Strength Dividend account — but the returns are largest for women navigating the hormonal and physiological transitions of midlife and beyond. This is the section for the woman who wonders if she has “missed her window,” or whether resistance training can really help with hot flashes, brain fog, or the muscle loss that seems to accelerate after 50. The answer, consistently and across multiple clinical bodies of evidence, is yes.
Managing Menopause Through Strength

Perimenopause (the transitional hormonal phase before menopause, typically beginning in the early-to-mid 40s) and menopause bring a cluster of symptoms that can feel overwhelming: hot flashes, sleep disruption, mood changes, weight gain — particularly around the abdomen — and accelerating bone loss. Estrogen (the primary female hormone that declines during perimenopause and menopause) plays a role in all of these. When it drops, the body loses a key protective signal for bone density, metabolic rate, mood regulation, and body composition.
Resistance training is one of the most clinically validated non-pharmacological responses to this transition.
A systematic review published in PMC (PubMed systematic review on strength training and menopause, 2026), analyzing multiple randomized controlled trials on strength exercises for menopausal symptoms, found that resistance training improves strength, physical activity levels, bone mineral density, and hormonal and metabolic markers in menopausal women. A related meta-analysis of 12 RCTs further found that resistance training reduced hot flash frequency compared to both no exercise and aerobic-only exercise groups (PubMed, 2022). Fat mass reductions of approximately 3 kg were observed compared to sedentary controls — a meaningful shift without any dietary change.
Resistance training is clinically supported as one of the most effective non-pharmacological interventions for managing menopausal symptoms — reducing hot flash frequency, supporting body composition, and protecting bone density simultaneously (PMC, 2026).
The mechanism here involves multiple pathways. Muscle tissue itself produces hormonal signals (called myokines) that improve insulin sensitivity and reduce systemic inflammation — both of which worsen during the menopausal transition. Strength training also directly addresses sarcopenia (the medical term for age-related muscle loss that affects most women after 50 without intervention) — a process that accelerates after estrogen decline.
The 2026 NHLBI finding adds an important note: women may realize greater proportional health benefits from exercise than men — meaning the dose required to achieve meaningful benefit is actually lower for women (NHLBI, 2026). This is genuinely encouraging news for anyone who feels overwhelmed by the prospect of starting.
Does Lifting Increase Estrogen?
Resistance training does not directly or dramatically increase estrogen levels, but it meaningfully modulates the hormonal environment in ways that support estrogen’s protective functions. Regular strength training reduces cortisol (the stress hormone that competes with sex hormone production), improves insulin sensitivity, and decreases systemic inflammation — all of which support more stable hormonal signaling during perimenopause and menopause. A systematic review (PubMed systematic review on strength training and menopause, 2026) found that resistance training improved hormonal and metabolic markers in menopausal women across multiple randomized controlled trials. The practical outcome: fewer hot flashes, better mood regulation, more stable energy, and improved body composition — even without directly raising estradiol (the primary form of estrogen) levels. Women on hormone replacement therapy should discuss exercise programming with their prescribing physician.
Protecting brain health and cognition is the next benefit — and one of the most compelling reasons to begin resistance training before symptoms appear.
Protecting Brain Health and Cognition

Women face a disproportionate risk of dementia: two-thirds of all dementia cases occur in women, with approximately double the lifetime risk compared to men (PMC, 2026). Perimenopause appears to represent a critical intervention window — the hormonal transition negatively impacts the female brain and may contribute to this elevated long-term risk.
Resistance training offers a meaningful and evidence-supported layer of protection. A 2026 PMC study of perimenopausal and early postmenopausal women found significant improvements in cognitive flexibility after nine months of twice-weekly resistance training, along with non-significant improvements in processing speed, inhibitory control, and verbal memory (PMC, 2026). A separate 24-week randomized controlled trial found that resistance training prevented gray matter atrophy in the hippocampus and precuneus — brain regions directly associated with memory and Alzheimer’s disease — while control subjects showed significant volume decreases in the same regions (PMC, 2026).
Resistance training protects the hippocampus — the brain’s primary memory center — against age-related atrophy, offering a clinically meaningful layer of cognitive defense for women at every life stage (PMC, 2026).
The mechanism is multi-pathway: resistance training increases blood flow to the brain, elevates BDNF (brain-derived neurotrophic factor — a protein that supports the growth and maintenance of neurons), reduces inflammatory markers associated with neurodegeneration, and improves insulin sensitivity in brain tissue. You do not need to understand each mechanism to benefit from it — but understanding that lifting weights changes your brain biology helps explain why the cognitive data is so compelling.
For women in their 40s and 50s navigating brain fog, word-finding difficulties, or concentration issues during the menopausal transition, this research offers practical encouragement. Research indicates 2–3 sessions per week are sufficient to produce measurable cognitive benefits — the same frequency that drives bone and metabolic improvements.
Starting resistance training after 50 is the natural next question — and the answer is more encouraging than most women expect.
Starting Resistance Training After 50
The most common concern among women in their 50s, 60s, and beyond is some version of: “Is it too late?” The clinical answer is unambiguous — no. Muscle responds to resistance training at any age. Studies confirm meaningful strength and muscle mass gains in adults in their 60s, 70s, and even 80s with progressive resistance programs. The NHS physical activity guidelines support resistance training for all age groups, including older adults, with appropriate load progression and supervision.
What does change after 50 is the approach. Recovery takes longer — 48–72 hours between sessions targeting the same muscle group is appropriate. Starting loads should be lighter, with emphasis on movement quality over weight lifted. The bone-loading benefits of resistance training are arguably more important after 50, given that bone loss accelerates sharply in the postmenopausal years. The LIFTMOR trial, notably, was conducted specifically in postmenopausal women with low bone mass — the very demographic many trainers historically told to avoid heavy lifting.
The Strength Dividend accrues at every age — and the returns for women who begin resistance training after 50 are among the highest of any demographic, precisely because the need is greatest.
Practical starting points after 50: bodyweight exercises (chair squats, wall push-ups, resistance band rows) build the movement patterns before external load is added. A certified personal trainer with experience in older adult fitness or physical therapy is an excellent first resource. Aim for 2 sessions per week, 20–30 minutes each, for the first 6–8 weeks. Progress only when form feels stable and confident — not on a fixed timeline.
Beginner’s Roadmap: First Steps

Most women who want to start resistance training face a specific barrier: they do not know what “enough” looks like. How many days? How many sets? What do they eat? These are the questions that keep a woman browsing Pinterest routines for months without ever starting. This section gives you clear, evidence-backed frameworks — so you can begin this week.
How Many Days a Week to Train?
The U.S. Department of Health and Human Services Physical Activity Guidelines for Americans recommend that adults perform muscle-strengthening activities targeting all major muscle groups on 2 or more days per week (HHS / ODPHP, 2018 guidelines, current as of 2026). This is the minimum threshold for health benefit — and for beginners, it is the right place to start.
A 2026 PMC review of minimal-dose resistance training strategies confirmed that 2–3 sessions per week with 8–10 exercises per session produces statistically significant improvements in muscle strength and mass in previously untrained adults (PMC, 2026). A separate meta-analysis found that 2 sessions per week represented the optimal frequency for the lowest cardiovascular and all-cause mortality risk in dose-response analyses — and that higher frequencies (4 or more times weekly) provided no additional cardiovascular benefit (PMC, 2020).
For beginners: 2–3 sessions per week is both the clinical minimum for health benefit and the practical maximum for sustainable recovery in untrained women.
Here is what a sensible beginner week looks like:
- Monday: Full-body resistance session (30–40 minutes)
- Wednesday: Rest or light walking
- Thursday or Friday: Full-body resistance session (30–40 minutes)
- Weekend: One optional session OR active rest (walking, yoga, stretching)
As your fitness improves over 8–10 weeks, you can progress to 3 sessions per week, or split upper and lower body across separate days. The key principle: allow at least one full rest day between sessions that target the same muscle groups.
The 3-3-3 Rule for Beginners
If the phrase “resistance training program” feels overwhelming, the 3-3-3 rule strips the complexity down to a structure a beginner can actually follow. In its most beginner-friendly form, the 3-3-3 rule means:
- 3 strength sessions per week
- 3 compound exercises per session (movements that work multiple muscle groups at once — think squat, push-up, row)
- 3 sets per exercise
That is your entire framework. Nine working sets per session. Two to three sessions per week. Done.
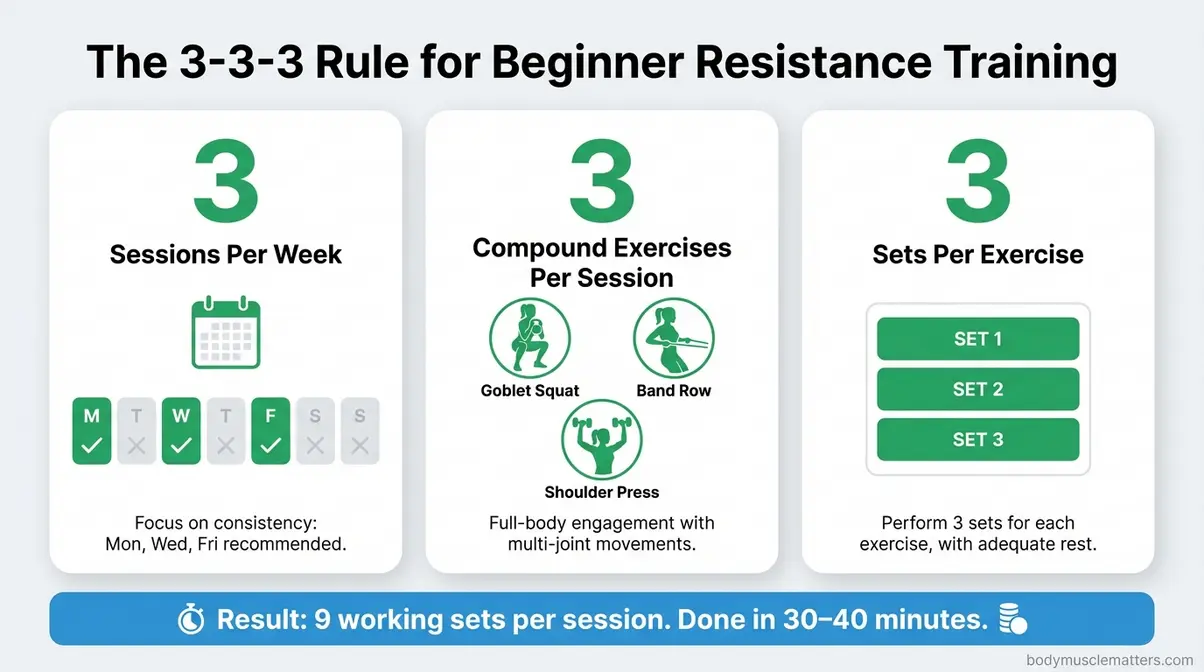
Caption: The 3-3-3 rule reduces beginner overwhelm to a single decision per session — choose 3 compound movements, do 3 sets each, three times a week.
A sample beginner session using the 3-3-3 rule:
- Goblet squat (works quads, glutes, core) — 3 sets of 10–12 reps
- Resistance band row (works upper back, biceps, rear shoulders) — 3 sets of 10–12 reps
- Dumbbell shoulder press or push-up (works chest, shoulders, triceps) — 3 sets of 8–10 reps
Rest 60–90 seconds between sets. Use a weight where the last 2 repetitions feel genuinely challenging — not impossible, but not comfortable either. As those reps become easier over 2–3 weeks, increase the resistance slightly. This principle is called progressive overload — it is how your body is forced to keep adapting.
The 3-3-3 rule works because it is repeatable and sustainable. Common concerns reported by beginners — “I don’t know what to do,” “I spend too long in the gym,” “I forget my routine” — all dissolve when the framework is this simple. For more structured guidance, review the 3-3-3 rule and other beginner gym routines.
The 30-30-30 Rule Explained
The 30-30-30 rule is a morning routine that pairs nutrition and movement to support fat loss and metabolic health. The format:
- Eat 30 grams of protein within 30 minutes of waking up
- Follow it with 30 minutes of low-intensity steady-state exercise (walking, light cycling, yoga)
The concept, popularized by author Timothy Ferriss and widely discussed by registered dietitians, is built on established nutrition and exercise science — not a single clinical trial designed to test the specific sequence. The protein component has the strongest evidence: eating a high-protein breakfast stabilizes blood sugar, reduces mid-morning cravings, and supports muscle protein synthesis (Stanford Lifestyle Medicine, 2026). Research consistently shows that distributing protein intake throughout the day — starting at breakfast — supports better body composition outcomes than back-loading protein at dinner.
The exercise component contributes toward the CDC strength training guidelines of 150 minutes of moderate aerobic activity per week while keeping cortisol levels low in the morning (Cleveland Clinic’s review of the 30-30-30 rule, 2026).
The 30-30-30 rule works as a morning anchor habit — the protein breakfast reduces cravings throughout the day, and the low-intensity movement builds a consistent exercise identity without overwhelming the beginner.
Thirty grams of protein at breakfast looks like: 4 large eggs (24g) plus a small Greek yogurt (6g); or Greek yogurt (15–20g) plus a protein shake (10–15g); or cottage cheese (20g) plus eggs (12g). Consult your physician or registered dietitian before making significant dietary changes, particularly if you have kidney health concerns or metabolic conditions.
The 30-30-30 rule is not a substitute for resistance training sessions — it is a complement to them, particularly for women who want a structured morning ritual alongside their gym days.
Protein for Women Who Train
Protein is the single most important nutritional variable for women beginning resistance training. Here is the practical breakdown:
| Life Stage / Activity Level | Recommended Protein | Daily Example (65kg woman) |
|---|---|---|
| Sedentary adult (baseline) | 0.8 g/kg body weight | ~52g/day |
| Actively strength training | 1.2–1.7 g/kg body weight | ~78–110g/day |
| Women over 50 building muscle | 1.4–2.0 g/kg body weight | ~91–130g/day |
| Post-workout recovery | 15–25g within 2 hours | Greek yogurt + protein shake |
Sources: UCLA Health (2026), government protein guidelines for muscle health (ACL/HHS), Mayo Clinic Health System (2026), Mass General Brigham (2026), Stanford Lifestyle Medicine (2026).
The higher end of the range — 1.6–2.0 g/kg — applies to women actively trying to build lean muscle, particularly those over 50 whose muscle protein synthesis response is slightly blunted compared to younger adults. Spreading protein across 3–4 meals produces better muscle-building outcomes than consuming most of it in one sitting.
Practical protein sources: eggs, Greek yogurt, cottage cheese, chicken breast, canned salmon, lentils, edamame, and protein powder. Resistance training without adequate protein is like saving money without depositing it — the work is real, but the compounding cannot happen.
Equipment: Dumbbells vs. Bands
You do not need a gym membership to begin. Here is a straightforward comparison of your two best beginner options:
| Equipment | Cost | Portability | Best For | Limitations |
|---|---|---|---|---|
| Resistance bands | $10–$30 | Excellent | Travel, home, rehabilitation | Harder to progressively overload |
| Adjustable dumbbells | $50–$150 | Moderate | Home gym, wide exercise range | Higher upfront cost |
| Fixed dumbbells (set) | $30–$100 | Low | Gym use, specific weights | Not adjustable |
| Gym membership | $20–$80/month | N/A — attend gym | Full equipment variety, classes | Requires travel, can feel intimidating |
For women who are apprehensive about entering a gym, resistance bands are the lowest-friction starting point. A set of three bands (light, medium, heavy) covers nearly every beginner exercise: rows, bicep curls, shoulder press, lateral walks, deadlifts, chest press. As confidence and strength grow, adjustable dumbbells extend the range of exercises and make progressive overload easier to manage.
If you do choose the gym, research suggests that arriving during off-peak hours (early morning or mid-afternoon on weekdays) significantly reduces the intimidation factor. Many gyms offer free orientation sessions — take them. Asking a staff member to demonstrate equipment use is normal, expected, and one of the smartest first moves a beginner can make.
Before You Begin: Safety and Common Mistakes
A cautionary note before the first session: the most common beginner injuries are not from lifting too heavy — they are from moving incorrectly with any weight at all. The guidance in this section will help you start smart.
Common Mistakes to Avoid When Starting
1. Skipping the warm-up. Five to ten minutes of light movement — dynamic stretches, arm circles, bodyweight squats — prepares joints and connective tissue for load. Starting cold is where most beginner strains happen.
2. Going too heavy, too soon. The goal of the first 2–4 weeks is movement quality, not weight load. If your form breaks down before you complete your reps, the weight is too heavy.
3. Inconsistent training frequency. One session every two weeks produces no meaningful adaptation. The 2 sessions per week minimum exists because consistency, not intensity, drives results for beginners.
4. Neglecting recovery. Muscle is built during rest, not during the session. Sleeping fewer than 7 hours per night and training every day without rest days impairs both recovery and results.
5. Holding your breath. Exhale during exertion (the lifting phase), inhale during the easier phase. Holding breath during effort raises blood pressure acutely — a concern for anyone with cardiovascular considerations.
6. Comparing your session to others’. The weights section contains athletes who have trained for years. Your only benchmark is your own previous session.
For a deeper walkthrough of form cues and beginner-safe progressions, see our comprehensive guide to developing functional strength.
When to Consult a Doctor First
Resistance training is safe for the vast majority of women — but certain circumstances call for a physician’s clearance before beginning.
Speak with your doctor before starting resistance training if you:
- Have been diagnosed with osteoporosis, osteopenia, or a fragility fracture (you may need supervised, specialized programming)
- Have a cardiovascular condition, including high blood pressure, heart disease, or arrhythmia
- Are pregnant or in the early postpartum period (12 weeks postpartum minimum before resuming loaded training without clearance)
- Have joint replacements, chronic joint pain, or herniated discs
- Have been sedentary for more than a year and are over the age of 60
- Have Type 1 or Type 2 diabetes, where exercise affects blood glucose management directly
This is not a list designed to discourage you — it is a checklist designed to protect you. For the vast majority of readers, a brief conversation with a GP or family physician is all that is needed to begin with confidence. A certified personal trainer with experience in medical fitness or physical therapy can also help design a program appropriate to your health history.
The risk of not exercising — for bones, heart, cognition, and metabolic health — significantly exceeds the risk of beginning a supervised, progressive resistance training program at any age.
Frequently Asked Questions
Why Resistance Training Matters
Resistance training is essential for women because it addresses the biological changes that no other form of exercise can fully reverse. After age 30, women lose 3–8% of muscle mass per decade without strength training, which drives metabolic slowdown, bone loss, and declining functional capacity (PMC, 2009). Clinical evidence links regular resistance training to reduced cardiovascular mortality risk, improved hormonal resilience during menopause, measurable cognitive protection, and enhanced mental health — all in a single intervention. Cardio supports heart health, but resistance training is the only modality that simultaneously builds bone, raises resting metabolism, and preserves the muscle mass women need for long-term independence (NHLBI, 2026).
What is the 3-3-3 rule at the gym?
The 3-3-3 rule is a beginner workout framework built around three sessions per week, three compound exercises per session, and three sets per exercise. It strips resistance training down to its most sustainable form: choose one lower-body, one upper-body push, and one upper-body pull movement. Perform each for 3 sets of 8–12 repetitions. Complete this routine twice or three times per week, resting at least one day between sessions. This structured simplicity makes it particularly effective for beginners who feel overwhelmed by more complex programming.
How Many Days a Week to Train?
Most women see meaningful benefit from 2–3 resistance training sessions per week, which aligns with U.S. Department of Health and Human Services guidelines. A 2026 PMC review of minimal-dose strategies found that 2 sessions per week produces significant improvements in strength and muscle mass in previously untrained adults (PMC, 2026). A dose-response meta-analysis identified 2 times per week as the frequency associated with the lowest cardiovascular mortality risk (PMC, 2020). More sessions are appropriate as fitness improves, but beginners should prioritize recovery — at least 48 hours between sessions targeting the same muscle groups.
Does It Help With Osteoporosis?
Yes — resistance training is one of the most clinically supported non-pharmacological interventions for both preventing and managing osteoporosis. The mechanical load placed on bones during resistance exercise activates osteoblasts (bone-forming cells), which deposit new bone mineral at the hip, spine, and wrist — the three sites most vulnerable to osteoporosis fractures (PMC, 2018). The LIFTMOR trial (Watson et al., 2018) demonstrated statistically significant bone mineral density improvements in postmenopausal women with low bone mass following a high-intensity resistance program. Women with diagnosed osteoporosis should work with a physiotherapist or certified trainer experienced in bone health before beginning.
What is the 30-30-30 rule for women?
The 30-30-30 rule is a morning routine involving 30 grams of protein within 30 minutes of waking, followed by 30 minutes of low-intensity exercise. It is designed to stabilize blood sugar, reduce morning hunger, and establish a consistent exercise habit. The protein component is well-supported: research shows that a high-protein breakfast reduces cravings throughout the day and supports muscle protein synthesis (Stanford Lifestyle Medicine, 2026). The exercise component contributes toward the recommended 150 minutes of weekly moderate aerobic activity. Most registered dietitians view it positively as a habit-formation tool, though no specific clinical trial validates the exact timing sequence.
The Strength Dividend Pays at Every Stage
For women at any age, the benefits of resistance training deliver one of the most comprehensive health returns available. Stronger bones reduce fracture risk. A raised resting metabolism makes body composition management sustainable without chronic restriction. Cardiovascular risk drops significantly — by up to 55% in women training 1–3 times per week (PMC, 2020). Menopausal symptoms become more manageable. Cognitive function is actively protected. And the mental health gains — the confidence, the calm, the capability shift — are often what beginners say they least expected and value most.
The Strength Dividend frames all of this as what it truly is: a compounding investment. Every session deposits into accounts of bone density, metabolic rate, hormonal resilience, and cognitive protection. Unlike most health interventions, the returns do not plateau — they compound. A woman who begins at 35 builds her dividend over 30 years. A woman who begins at 60 still builds it meaningfully over the decade ahead.
The first step is the same for both of them: start with 2 sessions per week, pick 3 compound exercises, do 3 sets each, and eat enough protein to support the work. Use the 3-3-3 rule as your framework. Add the 30-30-30 morning routine as your daily anchor. Speak with your doctor if any of the conditions in the safety section apply to you — and then begin.
You do not need perfect technique, expensive equipment, or a gym membership to collect your first deposit. You need to start — and the research on what happens when you do is among the most encouraging in all of health science.
