
⚠️ Medical Disclaimer: This article is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your doctor, pharmacist, or a licensed healthcare provider before starting any herbal supplement — especially if you take prescription medications, have a chronic health condition, or are pregnant or nursing.
Medically Reviewed:
You’ve seen the labels. “Boosts immunity.” “Lowers stress.” “Supports your heart.” Every time you reach for an herbal supplement, one question keeps nagging at you: is this actually working, or am I just burning through money?
The stakes are higher than wasted cash. Millions of people take herbal supplements daily without realizing that certain combinations with prescription medications — particularly statins and blood thinners — can quietly undermine their treatment or trigger dangerous side effects their bottle never mentions. Consumer skepticism about herbal supplement efficacy is surging, and for good reason: the marketing has far outpaced the clinical evidence.
This guide answers the central question: do herbal supplements actually work? We do this with something no competitor offers: real clinical trial data, an evidence tier classification you can apply to any herb you encounter, specific drug interaction warnings, and condition-targeted protocols for cortisol, SIBO, gut health, and more. We reviewed peer-reviewed clinical trials, NIH databases, and institutional health sources — and we cite every claim. Here’s what the science actually shows across six key areas: evidence overview, drug safety, stress and gut health, core nutrients, performance supplements, and weight management.
Whether herbal supplements actually work has a nuanced, evidence-based answer: some work exceptionally well, some show modest benefits, and many are unsupported by clinical trials.
- The Evidence Tier Framework: Herbs fall into Tier 1 (proven), Tier 2 (promising), or Tier 3 (hype) — use this to evaluate any supplement you’re considering
- Proven adaptogens: Ashwagandha reduces cortisol by 11–32.63% in stressed adults across multiple peer-reviewed RCTs (NIH systematic review, PMC10745833, 2023)
- Drug interactions are real: St. John’s Wort can measurably lower statin plasma concentrations, reducing their cholesterol-lowering effectiveness and increasing cardiovascular risk
- “Natural” ≠ Safe: Supplements aren’t FDA-approved before sale — liver toxicity from herbs like kava and comfrey is clinically documented
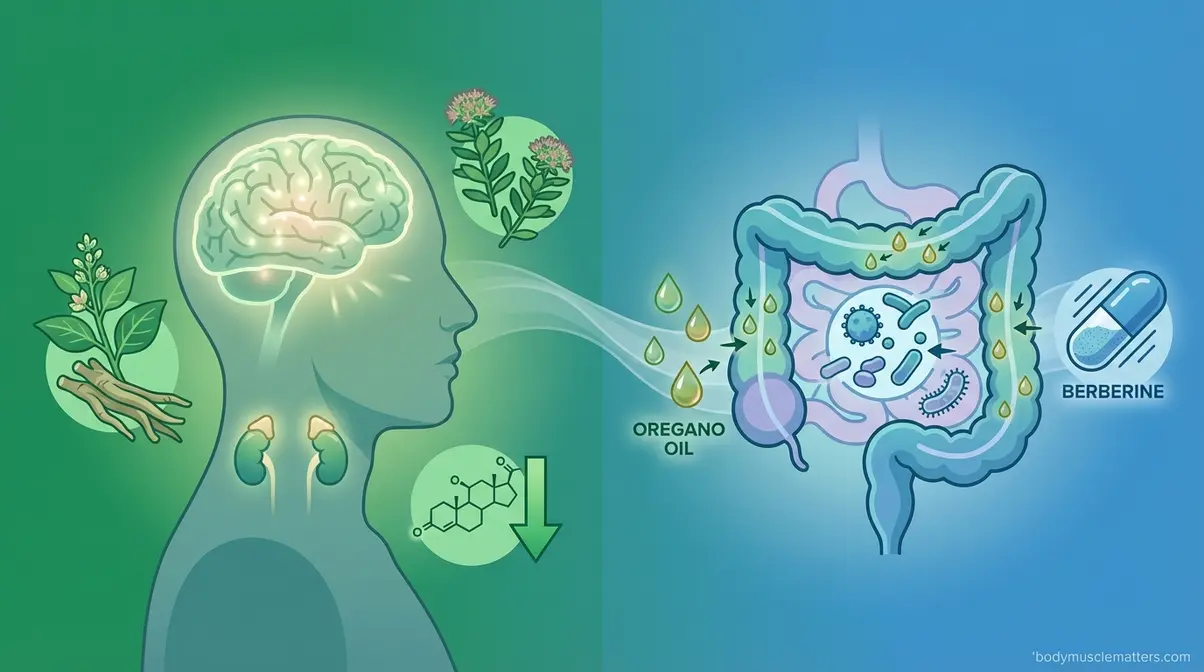
- Condition-specific herbs work: Herbal therapy (berberine + oil of oregano) matched the antibiotic rifaximin for resolving SIBO in a controlled clinical trial (NIH, PMC4030608, 2014)
The Science Behind Herbal Supplements
If you are asking, do herbal supplements actually work, the answer is yes — but only specific ones, for specific conditions, at clinically studied doses. The global herbal supplement market is projected to reach over $89–101 billion in 2026 (multiple industry analyses), yet not a single product requires proof of efficacy before reaching store shelves in the U.S. That asymmetry — enormous commercial scale, minimal clinical accountability — is precisely why you need a framework for reading the evidence, not just a label.
For this guide, our team reviewed peer-reviewed clinical trials, NIH and PubMed databases, and institutional health sources. We cite every specific claim. Here’s how to make sense of it.
What Is Herbal Medicine?
Herbal medicine is the practice of using plant-based compounds to support or improve health. You already know some: chamomile tea for sleep, ginger for nausea, garlic for heart health. What distinguishes herbal remedies from conventional pharmaceuticals is complexity — a pharmaceutical drug typically isolates one active compound at a precise dose, while an herbal extract contains dozens of bioactive compounds (the active ingredients in plants) that interact with the body simultaneously.
Think of it like this: caffeine in coffee affects your brain through one primary mechanism. Garlic extract, by contrast, contains allicin, quercetin, and organosulfur compounds that interact with the immune system, blood vessels, and lipid metabolism all at once. That complexity is both the promise and the problem. Beneficial interactions do occur — Hopkins Medicine overview documents how herbal compounds are used and categorized in traditional and modern medicine. But the same complexity makes standardizing doses and predicting outcomes far harder than with single-molecule drugs. This is exactly why clinical evidence varies so widely between herbs — and why you need a way to sort the evidence systematically.
Herbs With Strong Clinical Evidence
Not all herbs are equal. Peer-reviewed herbal efficacy research supports beneficial medicinal effects of specific botanicals while identifying compounds with inconsistent clinical outcomes. Here’s a preview of where common herbs actually fall, organized by evidence strength:
- Tier 1 — Strong clinical backing (multiple peer-reviewed RCTs):
- Ashwagandha — cortisol/stress reduction with specific, replicated percentage data
- Oil of Oregano — antimicrobial activity matching a prescription antibiotic for SIBO
- Lactase enzyme — clinically validated digestive enzyme replacement
- Iron supplementation — well-established nutrient repletion with documented absorption mechanisms
- Tier 2 — Promising but mixed results:
- St. John’s Wort — positive outcomes in some depression trials, but carries serious drug interaction risks
- Maca Root — small studies suggest libido support; mechanism unclear
- Rhodiola Rosea — reduced fatigue in some trials; sample sizes often small
- Garlic — modest cardiovascular data; generally well-tolerated
- Tier 3 — Mostly marketing:
- Echinacea — multiple large RCTs show no significant benefit for cold prevention
- Generic “fat burner” blends — proprietary formulas with no independent RCT support
- Klotho supplements — marketed on longevity research but the protein cannot meaningfully survive oral digestion in supplemental form
Herbal supplements range from clinically proven (Ashwagandha reducing cortisol by up to 32.63%) to entirely unsupported — the difference lies entirely in the quality of the clinical trials behind them.
We’ll cover each category in depth below. But first, the framework that makes evaluating any new supplement simple.
The Evidence Tier Framework
The Evidence Tier Framework — a three-category system for evaluating how well any herbal supplement is supported by clinical research — is the organizing structure of this entire guide. Here’s how to apply it:
Tier 1 — Strong Clinical Evidence: Supported by multiple independent, peer-reviewed randomized controlled trials (RCTs — the gold standard of clinical testing, where participants are randomly assigned to receive either the supplement or a placebo, with neither group knowing which they received). Results are consistent across different studies and populations. Examples: Ashwagandha, Lactase enzyme, Oil of Oregano (for SIBO), Iron supplementation.
Tier 2 — Promising but Mixed: Some positive trial data exists, but results are inconsistent or studies are small and short-term. These herbs may genuinely help — but the evidence isn’t strong enough to rely on them alone, especially for serious conditions. Examples: St. John’s Wort (depression), Rhodiola Rosea (stress), Garlic (cardiovascular), Maca (libido).
Tier 3 — Mostly Marketing: Supported by traditional use, animal studies, or single poorly controlled trials. No significant, independent human RCTs confirm the marketed claims. Examples: Echinacea, most “fat burner” blends, Klotho supplements.
The chart below shows where common herbs fall in the Evidence Tier Framework.
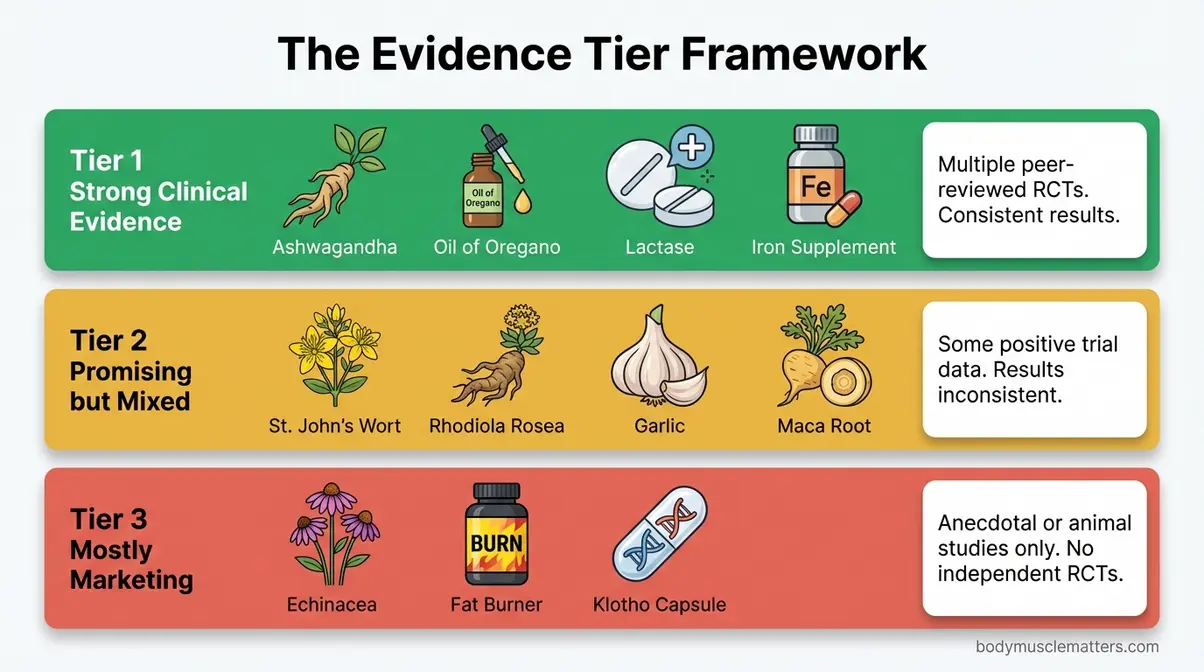
Caption: The Evidence Tier Framework classifies 15+ commonly used herbal supplements by the strength of their clinical trial support — from Tier 1 (multiple peer-reviewed RCTs) to Tier 3 (primarily traditional or anecdotal use).
Most well-known herbs fall into Tier 2 — meaning they may help, but the evidence isn’t strong enough to replace proven medical treatments. Keep this framework in mind throughout every section that follows.
Drug Interactions and Liver Toxicity
“Natural doesn’t always mean safe. Supplements can have side effects or interact with medicines.”
The most dangerous myth about herbal supplements is that being “natural” makes them safe. As medical authorities consistently confirm, supplements can cause measurable liver injury and reduce the effectiveness of critical medications — including the statins that millions of people depend on for cardiovascular protection. This is a statin warning worth understanding in detail before you buy anything off a supplement shelf.
Herbs That Interfere With Statins
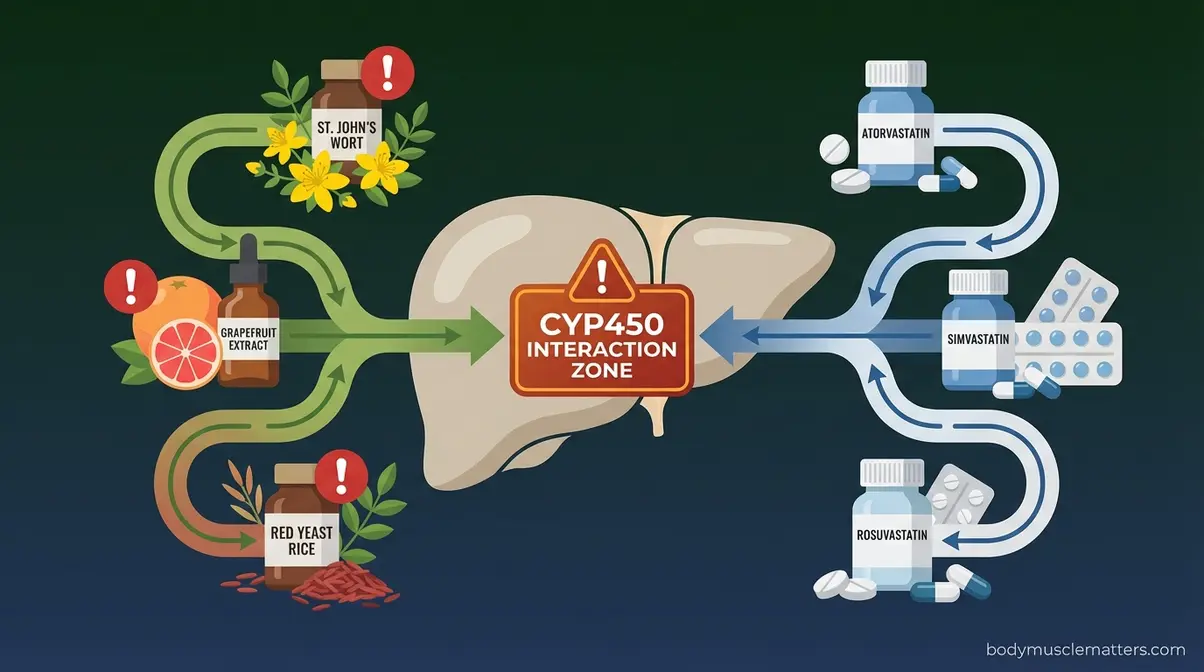
Your liver processes both prescription drugs and herbal compounds through a shared metabolic pathway called the CYP450 enzyme system — the liver’s processing lane for nearly all drugs and supplements. When two substances compete for the same CYP450 enzymes, one of two dangerous things happens: your statin levels can drop (reducing its cholesterol-lowering power) or spike (increasing toxicity risk). Think of it as two cars trying to use the same freeway lane — one will be slowed down or pushed into dangerous territory.
NIH research on herb-statin interactions documents that herbal materials like St. John’s Wort can decrease the plasma concentration (the amount of the drug actively circulating in your blood) of statin medications, potentially rendering them less effective in the body (NIH, 2015).
St. John’s Wort can significantly decrease the plasma concentration of statin medications — potentially reducing their cholesterol-lowering effectiveness and increasing cardiovascular risk. (NIH, PMC4593660)
The table below lists specific herbs with documented statin interactions. Verify your supplement against it before combining anything with a cholesterol medication.
| Herb | Interaction with Statins | Risk Level | What Happens |
|---|---|---|---|
| St. John’s Wort | Decreases statin plasma levels | 🔴 HIGH | Statin becomes less effective at lowering cholesterol |
| Chinese Skullcap | Decreases statin blood levels | 🔴 HIGH | Reduced cardiovascular protection |
| Grapefruit (extract) | Dramatically increases simvastatin by ~3.6x | 🔴 HIGH | Dangerous statin overdose risk |
| Red Yeast Rice | Contains natural lovastatin compound | 🔴 HIGH | Compounded statin effect; unpredictable dosing |
| Berberine | May enhance or reduce statin effect | 🟡 MODERATE | Unpredictable interaction; monitor closely |
| Milk Thistle | May alter statin metabolism via CYP3A4 | 🟡 MODERATE | Possible reduced liver clearance |
| Garlic (high dose) | May mildly affect lipid metabolism | 🟡 MODERATE | Possible additive lipid effect — generally tolerable |
| Coenzyme Q10 | May interact with statin muscle metabolism | 🟡 MODERATE | Unclear interaction; often taken together therapeutically |
| Chaparral | Severe hepatotoxicity risk | 🔴 HIGH | Amplifies statin liver stress significantly |
| Comfrey | Contains liver-damaging pyrrolizidine alkaloids | 🔴 HIGH | Life-threatening liver damage risk |
| Valerian Root | Inhibits CYP3A4 enzyme | 🟡 MODERATE | May slow statin clearance; increased exposure |
| Echinacea | Inhibits CYP3A4 at high doses | 🟡 MODERATE | Possible statin plasma level increase |
| Licorice Root | Affects aldosterone and drug metabolism | 🟡 MODERATE | Blood pressure and statin interaction risk |
| Turmeric (high dose) | CYP3A4 inhibition at supplemental doses | 🟡 MODERATE | May slow statin metabolism |
| Goldenseal | Strong CYP3A4 and CYP2D6 inhibitor | 🔴 HIGH | Significant statin accumulation risk |
Sources: NIH (PMC4593660); consult your pharmacist for your specific statin brand.
A real-world example: if you’re taking atorvastatin and decide to add St. John’s Wort for low mood, your cholesterol medication may quietly stop working — with no obvious symptoms until your next blood test. Regarding the common question about vitamin D and statins: a JAMA Cardiology randomized clinical trial tracking over 2,000 participants found that vitamin D supplementation did not prevent statin-associated muscle symptoms or reduce statin discontinuation rates (JAMA Cardiology, 2022), making it a Tier 2 combination at best.
The Hidden Liver Toxicity Risk
Hepatotoxicity — liver toxicity, meaning direct damage to liver cells caused by a chemical compound — is documented in several commonly sold herbal products. The NIH LiverTox database on supplement-induced liver injury confirms that herbal and dietary supplements are increasingly implicated in drug-induced liver injury cases, with toxic profiles sometimes matching prescription medications (NIH LiverTox).
These are the specific herbs with well-documented liver damage risk:
- Chaparral (Larrea tridentata): Nordihydroguaiaretic acid (NDGA) causes direct liver cell damage. Severe cases have required liver transplants.
- Comfrey: Contains pyrrolizidine alkaloids that permanently damage liver blood vessels (veno-occlusive disease). Banned for internal use in many countries.
- Kava: Linked to liver failure cases in Europe — Germany, the UK, and Switzerland banned or restricted it in the early 2000s after over 40 reported cases of liver-related illness (FDA Scientific Memorandum, 2020). The FDA issued a consumer advisory but stopped short of a full ban; kava remains available in the U.S.
- Coltsfoot: Contains hepatotoxic pyrrolizidine alkaloids similar to comfrey.
- Pennyroyal: The essential oil in particular has caused acute liver failure and death in documented cases.
The “unlisted prescription drugs” problem compounds this risk. Some commercially sold supplements have been found to contain unlisted active pharmaceutical ingredients — synthetic compounds, steroids, and stimulants that the label never declares. The FDA’s Tainted Products Database has issued warnings about specific brands found to contain undeclared prescription-strength compounds. Always check it before buying.
Before You Take Any Herbal Supplement — Safety Checklist:
- Check the FDA Tainted Products Database for your specific brand
- Tell your doctor and pharmacist every supplement you take — including vitamins and herbs
- Look for third-party testing seals (USP, NSF International, or ConsumerLab)
- Avoid any product claiming to “replace” a prescription medication
- If you take statins, blood thinners, or immunosuppressants, get pharmacist approval before adding any herb
The FDA vs. European Regulation Gap
Under the Dietary Supplement Health and Education Act (DSHEA) of 1994, the U.S. treats supplements as food, not drugs. Manufacturers do not need to prove safety or efficacy before a product reaches store shelves. The FDA only intervenes after a product is already for sale and complaints have been filed. In practice, when you buy a supplement in the U.S., you are essentially participating in an uncontrolled safety study.
Europe operates differently. The Traditional Herbal Medicinal Products Directive (THMPD) requires herbal medicines to be registered before they can be sold, with evidence of safety and acceptable quality — although the efficacy bar is lower than for pharmaceuticals. A product must have documented use for at least 30 years (including 15 in the EU) before registration.
The contrast is stark. Kava supplements were banned in Germany, the UK, Switzerland, and France after documented liver failure cases. In the U.S., kava remained on shelves with only an FDA advisory, allowing consumers who hadn’t heard about the European regulatory action to keep purchasing it.
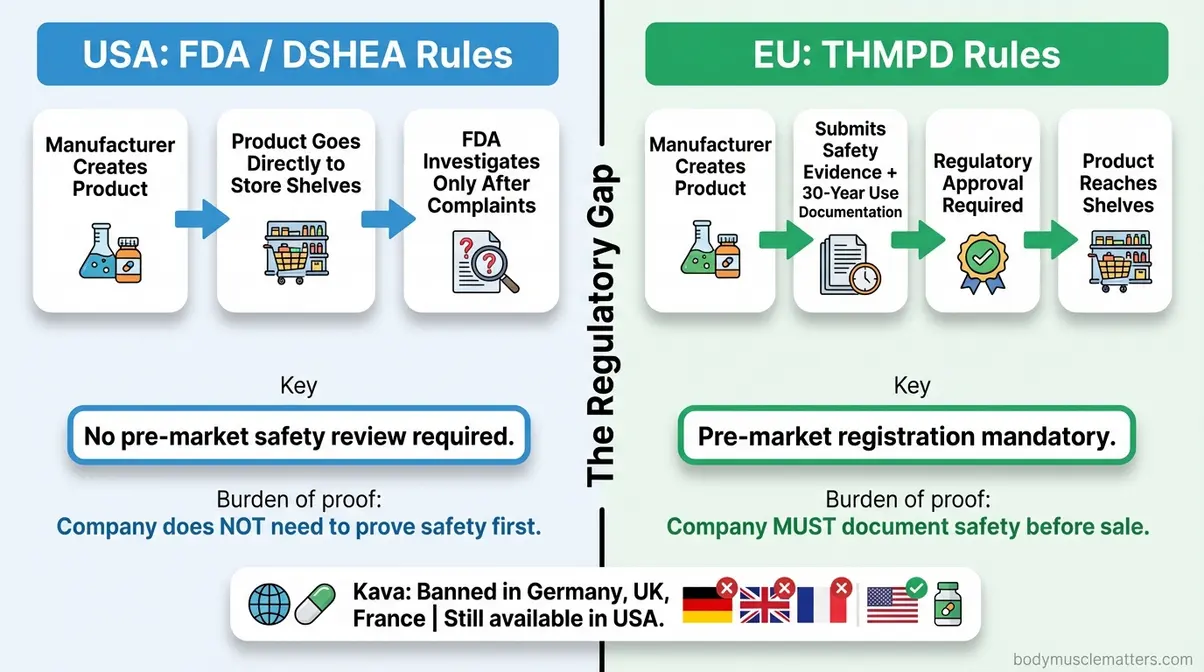
Caption: Under U.S. DSHEA rules, supplements reach shelves without pre-market safety review. The EU’s THMPD requires documented safety evidence before any herbal product can be sold.
Herbs for Stress and Gut Health
Institutional competitors — Hopkins, Mayo Clinic, Cleveland Clinic — have published nothing on herbal protocols specifically for cortisol reduction or Small Intestinal Bacterial Overgrowth (SIBO). This is where the clinical evidence is most actionable for the people who need it most.
Adaptogens That Lower Cortisol
Adaptogens are herbs that help the body manage stress by modulating the stress-response system — specifically the HPA axis (hypothalamic-pituitary-adrenal axis), the body’s central alarm system for stress. Think of the HPA axis as a smoke detector that fires when you’re stressed and is supposed to quiet down once the stressor passes. In chronic stress, it stays stuck in alarm mode, keeping cortisol elevated around the clock. Adaptogens help the system reset faster.
Ashwagandha (Withania somnifera), an adaptogenic herb central to Ayurvedic medicine for over 3,000 years, is the clearest Tier 1 example in this category. A study showing ashwagandha reduces cortisol by up to 32% — specifically, a peer-reviewed NIH systematic review of nine RCTs — demonstrated that Withania somnifera supplementation lowered plasma cortisol levels in stressed healthy individuals by 11% to 32.63% across studies (NIH, PMC10745833, 2023). The studied dose range is 300–600mg of root extract daily for 8 weeks. To put that in perspective: a 30% cortisol reduction is comparable to what you’d achieve through a consistent daily exercise program — delivered in supplement form, without a gym.
Rhodiola Rosea, an adaptogenic herb native to cold mountainous regions of Europe and Asia, sits firmly in Tier 2. Studies show reduced fatigue and improved stress resilience, but sample sizes are often small and results are inconsistent across populations. It’s worth trying for stress management alongside lifestyle changes, but don’t rely on it as a primary intervention.
How do you flush cortisol out of your body? The direct answer: there is no supplement that “flushes” cortisol directly. Cortisol is metabolized by the liver through natural biological processes. The most evidence-backed approaches are sleep optimization (7–9 hours), consistent aerobic exercise, and adaptogenic herbs like Ashwagandha — which modulate how much cortisol your HPA axis produces in the first place, rather than flushing existing cortisol. Ashwagandha’s mechanism is reducing the HPA axis’s alarm sensitivity, not accelerating cortisol clearance.
What vitamin deficiency is associated with high cortisol? Vitamin D deficiency is correlated with elevated cortisol in some observational studies. The relationship appears to be bidirectional — chronic stress depletes Vitamin D levels, and low Vitamin D may impair the body’s ability to regulate cortisol. However, this evidence is correlational, not causal. If you’re chronically stressed and have low Vitamin D (confirmed by bloodwork), supplementing Vitamin D is a reasonable starting point alongside adaptogenic herbs — but don’t treat it as a standalone cortisol solution.
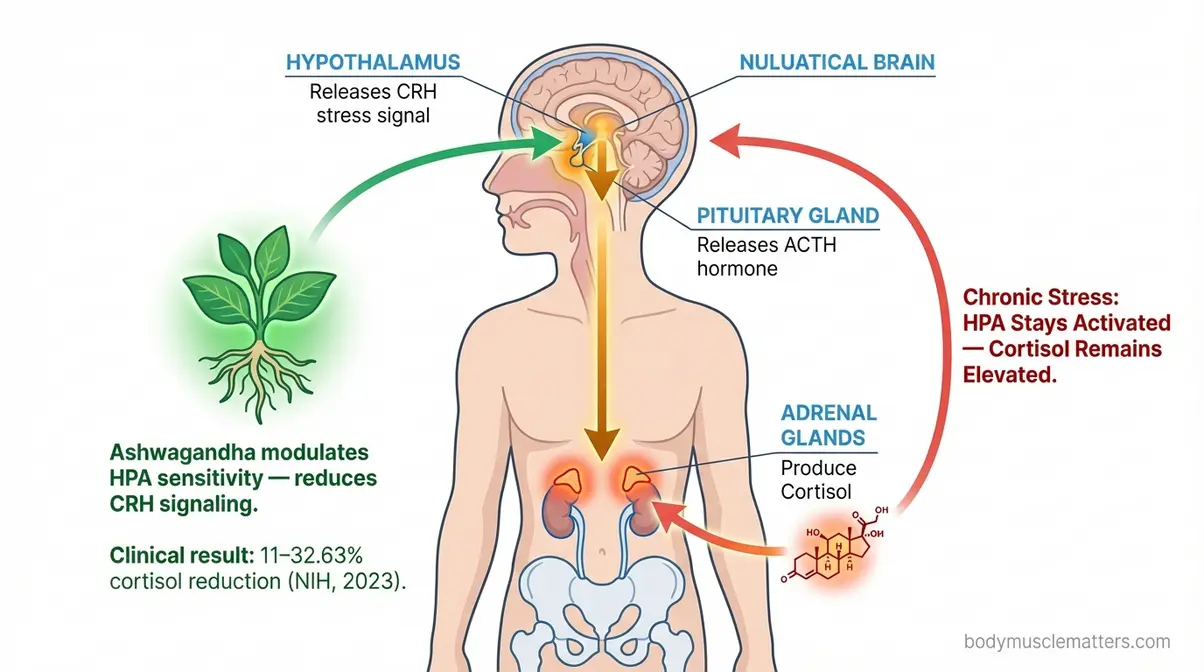
Caption: Ashwagandha modulates the HPA axis stress cascade — reducing cortisol production at its source rather than masking downstream symptoms.
Evidence-Based SIBO Protocols
Small Intestinal Bacterial Overgrowth (SIBO) is a condition in which excess bacteria colonize the small intestine, causing bloating, gas, and digestive distress. It affects an estimated 6–15% of the general population, and considerably higher rates in people with IBS. Common early signs include:
- Persistent abdominal bloating, especially after meals
- Excessive gas and flatulence
- Abdominal cramping or pain
- Alternating diarrhea and constipation
- Unexplained brain fog or fatigue
Rifaximin — a prescription antibiotic currently considered the standard medical treatment for SIBO — has a herbal challenger with clinical backing. Oil of Oregano contains carvacrol and thymol, two antimicrobial compounds with documented activity against the bacterial species that overpopulate the small intestine in SIBO.
The NIH trial: herbal therapy matches rifaximin for SIBO found that herbal therapies containing berberine and oregano oil achieved SIBO remission in 46% of patients — compared to 34% for rifaximin at standard dosing — with no statistically significant difference between groups (NIH, 2014). In plain terms: herbal antimicrobials worked at least as well as the prescription antibiotic. That is a Tier 1 finding and a significant one.
“Starve a SIBO” is user shorthand for the dietary component of herbal SIBO treatment — and the concept is clinically supported. Herbal antimicrobials like oregano oil work most effectively when paired with a low-FODMAP or elemental diet that removes fermentable carbohydrates, essentially starving the bacteria of their fuel source while the antimicrobials attack them directly. The dietary component is not optional; without it, bacterial regrowth is rapid.
A typical herbal SIBO protocol: 500mg of emulsified oil of oregano twice daily, combined with berberine (400–500mg twice daily), on a short-term low-FODMAP diet for 4–6 weeks. This should always be done under physician supervision — SIBO requires a confirmed diagnosis (via lactulose breath test), and herbal protocols should be monitored for response.
Herbs Shown to Support Nerve Health
Nerve health is one area where the Evidence Tier Framework applies cautiously — promising signals exist, but overclaiming would mislead you.
Turmeric/Curcumin is the most defensible option here. Curcumin (the primary active compound in turmeric) exerts anti-inflammatory effects via NF-kB pathway inhibition, which is relevant to neuropathic pain driven by chronic inflammation. It’s a Tier 2 herb for nerve support — the evidence is credible, but bioavailability (how much of the active compound your body actually absorbs and uses) is genuinely poor from standard turmeric powder. Pairing curcumin with piperine (an extract from black pepper) increases absorption by up to 2,000% according to some pharmacokinetic studies — if your curcumin supplement doesn’t contain piperine, you may be absorbing very little.
Ginkgo Biloba improves peripheral blood flow, which can benefit nerve function where poor circulation is the underlying driver. The evidence is Tier 2 for peripheral neuropathy — narrowly. Large dementia trials were negative. Do not use Ginkgo for cognitive decline; its specific credible application is peripheral circulation support.
Holy Basil (Ocimum sanctum) shows neuroprotective properties in animal models and has adaptogenic properties consistent with stress-related nerve tension. For humans, though, clinical evidence remains limited — borderline Tier 2/Tier 3 for nerve damage specifically. If you’re managing nerve damage from diabetes or chemotherapy, discuss curcumin supplementation with your neurologist. It carries enough anti-inflammatory data to warrant a conversation with your care team.
Core Nutrients and Digestive Blends
Some supplements work through clear, well-understood biological mechanisms — and iron and lactase enzyme are the best examples. Others leverage that trust to sell products with far less justification.
How Iron Supplements Actually Work
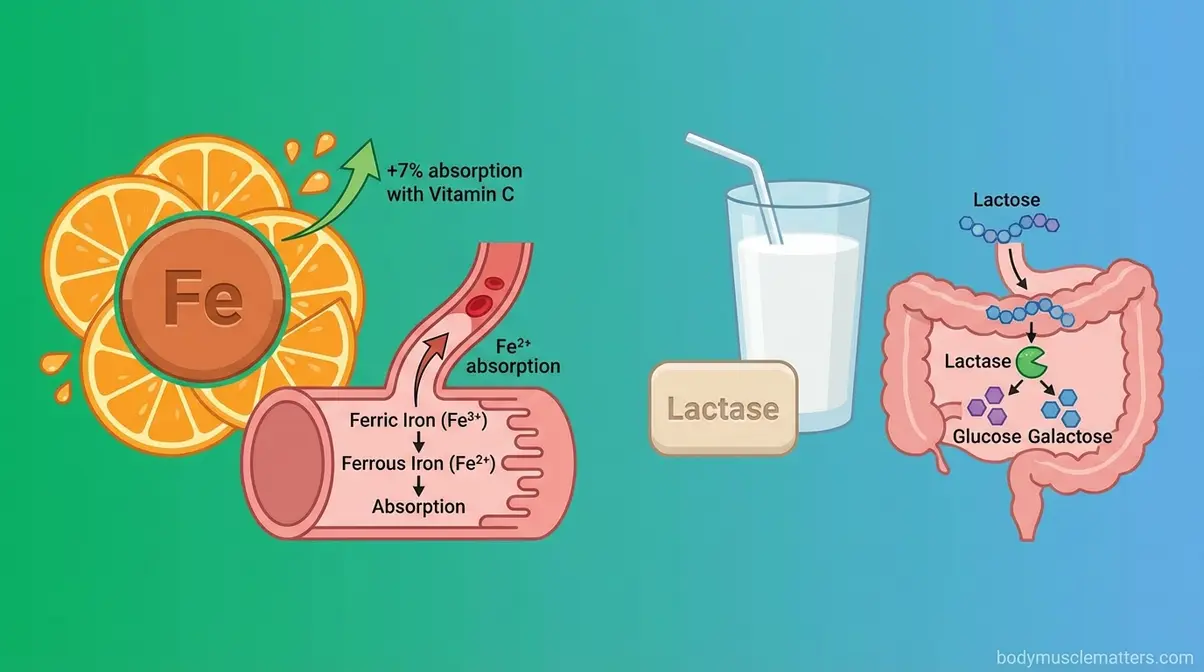
Iron supplements are oral preparations used to treat iron deficiency anemia (IDA), the most common nutritional deficiency worldwide. Understanding how iron absorption works helps you take it correctly — because most people don’t.
Iron enters the small intestine in its oxidized form (ferric iron, Fe³⁺). Before it can cross into the bloodstream, it must be converted to its absorbable form (ferrous iron, Fe²⁺). Vitamin C (ascorbic acid) drives this conversion directly. NIH research on vitamin C and iron absorption documents that iron absorption rates increase progressively as vitamin C intake rises — from less than 1% without vitamin C to over 7% with 1,000mg of vitamin C alongside the same iron dose (NIH, 2022). Without vitamin C, your body’s ability to convert and absorb iron is substantially constrained — meaning the supplement you paid for may be partially going to waste.
Three absorption mistakes most beginners make:
- Taking iron with coffee or tea: Tannins in both beverages chemically bind to iron and block absorption before it reaches the intestinal wall
- Taking iron with calcium supplements: Calcium and iron compete for the same intestinal transport proteins — separate them by at least 2 hours
- Taking iron on a completely empty stomach: Maximizes absorption in theory, but causes nausea for most people. The practical compromise: take with a small amount of vitamin C-rich food (orange juice works well)
Who genuinely benefits? People with confirmed iron deficiency anemia — diagnosed via bloodwork showing low ferritin and/or hemoglobin. Also: people with heavy menstrual periods, vegans and vegetarians (plant iron is non-heme and absorbs less efficiently), and frequent blood donors. Caution: excess iron is toxic. Never self-supplement iron without a blood test confirming deficiency first.
The Clinical Truth About Lactase
Lactase is an enzyme naturally produced in the small intestine that breaks down lactose, the sugar in dairy products. When your body doesn’t produce enough lactase, undigested lactose travels to the colon, where bacteria ferment it — producing the gas, bloating, and diarrhea that characterize lactose intolerance.
Supplemental lactase is a direct replacement therapy. Take an oral lactase tablet immediately before your first bite of dairy, and the enzyme is present in your digestive tract at exactly the moment it’s needed. This is mechanically elegant in a way most supplements are not — you’re supplying a specific missing biological catalyst at the precise point of need.
The clinical evidence is Tier 1. An NIH study on lactase supplementation found that orally supplemented lactase enzyme significantly reduces hydrogen breath excretion (a marker of bacterial fermentation in the colon) and gastrointestinal symptoms in patients with lactose intolerance (NIH, 2021). This is one of the cleaner supplement success stories because the mechanism is fully understood, the target population is well-defined, and the clinical results are consistent.
Practical guidance: take 1–3 tablets immediately before your first bite of dairy. The enzyme needs to be in your stomach simultaneously with the lactose. Don’t take it 30 minutes beforehand.
Does Balance of Nature Actually Work?
Balance of Nature is a commercially popular whole-food supplement brand that dehydrates and concentrates fruits and vegetables into capsules. Its marketing claims to provide the equivalent nutrients of multiple servings of produce.
The core problem: while whole-food concentrates do contain vitamins, minerals, and phytonutrients, bioavailability from dehydrated powders is generally lower than from fresh produce. Dehydration and processing alter phytonutrient structures, and some compounds that appear in laboratory tests of the powder may not survive the digestive process in usable form. More critically, there are no peer-reviewed, independent RCTs specifically studying Balance of Nature’s efficacy claims. Evidence tier: Tier 3 for its specific marketing claims — traditional food-form supplement with no clinical trial support.
The honest verdict: if you genuinely cannot eat enough fruits and vegetables, a whole-food supplement is probably better than nothing — but it is not equivalent to a whole-foods diet. The $60–$100/month price point is difficult to justify on the available evidence alone. A more evidence-supported use of that budget: frozen berries, spinach, and bell peppers have consistent and superior bioavailability compared to powdered concentrates, at a fraction of the cost.
Performance and Longevity Herbs

Most libido and performance supplements sold today fall into Tier 3 of the Evidence Tier Framework — with marketing budgets vastly exceeding their clinical evidence. A few exceptions exist, and they’re worth knowing precisely.
Do Libido Supplements Work?
The short answer: it depends on the cause of your low libido, and most products don’t address root causes at all.
Maca Root (Lepidium meyenii), an Andean root vegetable used as a libido and energy supplement, has several small studies suggesting it may improve sexual desire in both men and women. Evidence tier: Tier 2. The studies show positive signals, but sample sizes are small and the mechanism is not fully understood — it doesn’t appear to be hormonal. Don’t expect Maca to override testosterone deficiency or thyroid dysfunction.
Ashwagandha (already established as Tier 1 for cortisol) earns Tier 2 status for libido specifically. When low libido is stress-related — driven by chronically elevated cortisol suppressing testosterone and sex hormone binding — Ashwagandha has the most clinical backing of any herb in this category. If reducing cortisol improves hormonal balance, the libido benefit follows secondarily.
Here’s what most libido supplement labels won’t tell you: low libido can be caused by thyroid dysfunction, testosterone deficiency, medication side effects (SSRIs are a common culprit), or clinical depression. Herbal supplements cannot address these root causes. Before spending money on supplements, rule out medical causes with basic bloodwork — it’s a more efficient use of your healthcare dollar.
If your low libido is primarily stress-related, 300–600mg of Ashwagandha root extract daily has the best clinical backing. If it’s hormonal or medication-related, see your doctor before spending on supplements.
Do Shilajit Gummies Actually Work?
Shilajit is a resinous substance formed over centuries from decomposed plant matter in Himalayan rock formations, used in Ayurvedic medicine for energy, vitality, and male reproductive health. It contains fulvic acid and over 80 trace minerals. A 2016 randomized, double-blind, placebo-controlled clinical trial (n=75 men, aged 45–55) found that purified Shilajit resin (250mg twice daily for 90 days) significantly increased total testosterone by 20.45%, free testosterone by 19.14%, and DHEAS by 31.35% versus placebo (Andrologia, 2016, PMID: 26395129). Evidence tier for the purified resin form: Tier 2 — the data is promising but from a small single trial.
The gummy formulation is a different product entirely. Bioavailability — how much of a supplement’s active ingredient your body actually absorbs and uses — is the central issue. Shilajit gummies contain dramatically lower concentrations of active fulvic acid compounds than purified resin or standardized capsule extracts. The sugar and gelatin matrix of a gummy further impedes absorption of the active compound. No clinical trial has tested the gummy formulation specifically. Evidence tier for gummy-form Shilajit: Tier 3 — insufficient evidence to support the claimed testosterone and energy benefits at the doses these products deliver.
The practical takeaway: if you want to trial Shilajit based on available evidence, use a standardized resin or capsule extract from a third-party tested brand — not a gummy.
Gaming Supplements and Klotho
Gaming supplements — a category of nootropic and stimulant-based products marketed specifically to esports and gaming communities — are almost universally Tier 3. Most rely on caffeine (well-established for focus and reaction time at 100–200mg doses), combined with proprietary blends of unproven nootropics. Caffeine itself is Tier 1 for short-term cognitive performance. The rest of the formula typically isn’t.
Klotho is a protein associated with aging and longevity in research contexts — naturally produced by the body, and declining with age. The longevity research on klotho is genuinely interesting at the cellular biology level. The oral supplement market, however, is built on a fundamental biological problem: klotho is a large protein that does not meaningfully survive the digestive process to enter the bloodstream in supplemental form. You cannot increase your klotho levels by eating klotho. Evidence tier: Tier 3 — the underlying science is promising, the supplement form is not clinically supported. Watch this space for future delivery mechanisms (intranasal or IV), but skip the current oral products.
Weight Loss and Metabolism
Weight management supplements represent the most crowded and most misleading category in the herbal supplement market — and the place where the Evidence Tier Framework delivers the most protection for your wallet and your health.
Do Metabolism Boosters Work?
Most metabolism booster supplements are Tier 3. Products marketed as “metabolism boosters” or “thermogenics” typically combine caffeine, green tea extract (EGCG), and capsaicin — ingredients that do have modest evidence for marginally increasing metabolic rate (thermogenesis, or heat production) in the short term. The effect sizes in clinical trials are small: an increase of 50–100 calories per day at best, and this effect diminishes with regular use as the body adapts.
The practical reality: no supplement meaningfully replaces the caloric deficit and metabolic improvements driven by diet and exercise. When a product’s marketing claim is “boost your metabolism,” reach for the Evidence Tier Framework. Ask: what is the specific mechanism? What is the RCT evidence? What is the actual effect size in calories? Most products fail all three questions. Caffeine is the only consistent Tier 1 component in this category, and you don’t need a proprietary blend to get it.
Chia Seeds for Weight & Cholesterol
Chia seeds occupy an interesting position: they are a whole food with genuine clinical backing for specific outcomes — not a supplement in the traditional sense, but frequently marketed as one.
For weight management, the evidence is mixed (Tier 2). Chia seeds’ high soluble fiber content expands in the stomach, potentially increasing satiety. Several small trials show modest reductions in appetite and body weight, but effect sizes are not dramatic and results vary. They are most useful as a dietary addition that supports a caloric deficit, not as a standalone weight loss intervention.
For cholesterol, chia seeds have more consistent data. The soluble fiber (primarily mucilage) binds to bile acids in the intestine and promotes their excretion, which forces the liver to synthesize new bile acids from cholesterol — effectively pulling LDL cholesterol out of circulation. This mechanism is well-established for soluble fiber broadly.
What flushes cholesterol out of your body? The most evidence-backed approach is a combination of: soluble fiber (chia seeds, psyllium, oats) that binds bile acids; plant sterols/stanols that block cholesterol absorption in the intestine; and, where appropriate, prescription statins that inhibit cholesterol synthesis in the liver. No supplement “flushes” cholesterol instantly — the mechanism is gradual and dietary, not acute. Chia seeds are a Tier 2 adjunct to a heart-healthy diet, not a replacement for medical cholesterol management.
When Herbal Supplements Don’t Work
Mistakes That Stop Effectiveness
When asking, “do herbal supplements actually work?”, the Evidence Tier Framework reveals a pattern: even Tier 1 herbs fail when taken incorrectly. Here are the most common reasons evidence-backed supplements underperform:
1. Wrong dose or form. Ashwagandha’s clinical data is based on 300–600mg of standardized root extract — not raw powder, not tea, not a blend where ashwagandha is the 8th ingredient. Many products list “ashwagandha” on the label at doses with no clinical support. Always compare the supplement’s dose and extract standardization to the actual trial parameters.
2. Poor bioavailability not addressed. Curcumin without piperine. Shilajit in gummy form. Iron taken with coffee. These are all real-world delivery failures that make a Tier 1 ingredient perform like Tier 3.
3. Expecting supplement-speed results from slow biological processes. Ashwagandha’s cortisol reduction was measured at 8 weeks. Consistent iron supplementation requires 3–6 months to meaningfully restore ferritin stores. Impatience leads people to abandon supplements that were actually working.
4. Combining supplements with medications without checking interactions. St. John’s Wort silently reducing your statin’s effectiveness. Garlic at high doses affecting your blood thinner’s dose. These interactions produce no immediate symptoms — they show up in your next bloodwork or, in serious cases, much later.
5. Skipping third-party testing verification. A supplement’s label is not a guarantee of its contents. Third-party testing (USP, NSF, ConsumerLab) is the only way to verify that what’s on the label is actually in the bottle.
When to Choose Alternatives Instead
Herbal supplements are adjuncts — tools that work alongside lifestyle and medical treatment, not replacements for them. Choose alternatives in these specific scenarios:
When your condition requires a confirmed diagnosis first. SIBO herbal protocols work — but only if you actually have SIBO. Self-treating gut symptoms with herbal antimicrobials without a lactulose breath test can worsen dysbiosis if the diagnosis is wrong. Similarly, self-treating low energy or mood with adaptogens without checking thyroid function or CBC blood panels is guessing with your health.
When a prescription medication has superior safety and efficacy data. If you have Type 2 diabetes, metformin has decades of cardiovascular outcome data that berberine — despite promising mechanistic similarities — cannot currently match. Use berberine as a complement to medical care, not a replacement.
When you’re pregnant, nursing, or planning to become pregnant. Most herbal supplements have insufficient pregnancy safety data. The default position is avoidance unless a qualified healthcare provider has specifically reviewed the evidence and approved the supplement for your situation.
When symptoms are worsening despite supplementation. Give evidence-based supplements a fair trial period (8–12 weeks at the clinically studied dose). If symptoms are worsening or unchanged, the supplement is not the right intervention for your specific situation. Escalate to professional evaluation rather than adding more supplements.
Frequently Asked Questions
What herbal supplements interfere with statins?
Several common herbs interact dangerously with statins via the CYP450 liver enzyme system. St. John’s Wort poses the highest risk — it significantly decreases statin plasma concentrations, potentially making your cholesterol medication ineffective. Red Yeast Rice contains a natural statin compound, creating an unpredictable compounding effect. Grapefruit extract can increase simvastatin blood levels by approximately 3.6 times, raising overdose risk. Goldenseal and Chinese Skullcap are also high-risk. Always consult your pharmacist before combining any herb with a statin medication (NIH, PMC4593660).
What herb kills SIBO?
No herb “kills” SIBO permanently, but oil of oregano (containing carvacrol and thymol) has the strongest clinical evidence as an herbal antimicrobial for SIBO. A peer-reviewed NIH trial found herbal therapies including oregano oil and berberine achieved SIBO remission in 46% of patients — at least equivalent to the prescription antibiotic rifaximin (NIH, PMC4030608, 2014). Oil of oregano works most effectively when combined with a low-FODMAP diet that starves the bacteria simultaneously. Always confirm a SIBO diagnosis before starting any treatment.
What herbs are good for nerve damage?
For nerve damage support, curcumin (the active compound in turmeric) has the most clinically relevant evidence — its anti-inflammatory mechanism via NF-kB pathway inhibition is specifically relevant to neuropathic pain. Pair it with piperine (black pepper extract) to dramatically increase bioavailability. Ginkgo Biloba may support peripheral circulation-related neuropathy. Holy Basil shows early promise in animal models but lacks strong human trial data. None of these replace conventional neuropathy treatment — discuss curcumin supplementation with your neurologist as an adjunct to prescribed care.
Why can’t you take vitamin D with a statin?
The concern is not that vitamin D is dangerous with statins — it’s that the expected benefit may not materialize. A JAMA Cardiology randomized clinical trial of over 2,000 participants found that vitamin D supplementation did not prevent statin-associated muscle symptoms or reduce statin discontinuation rates (JAMA Cardiology, 2022). If you’re experiencing muscle pain on a statin and hoping vitamin D will help, the clinical evidence does not currently support that expectation. Discuss statin muscle symptoms directly with your doctor — there are other pharmacological and dose-adjustment strategies with better evidence.
Do herbal supplements actually work for weight loss?
When asking, “do herbal supplements actually work for weight loss?”, the truth is most weight-loss supplements do not deliver meaningful results as standalone interventions. Caffeine and green tea extract (EGCG) have modest evidence for marginally increasing metabolic rate, but effect sizes are small — typically 50–100 calories per day — and diminish with regular use. Soluble fiber from whole foods like chia seeds and psyllium has better evidence for satiety and LDL cholesterol reduction than any proprietary “fat burner” blend. No herbal supplement replaces a caloric deficit from diet and exercise. For weight loss, the Evidence Tier Framework consistently points to dietary and behavioral interventions, with herbal supplements at best playing a supporting role.
Conclusion
For health-conscious adults navigating a supplement market flooded with unverified claims, the honest answer to whether herbal supplements actually work is this: it depends entirely on which herb, which condition, and whether you’re using the Evidence Tier Framework to separate clinical reality from marketing. Ashwagandha delivers a clinically meaningful cortisol reduction of 11–32.63% (NIH systematic review, 2023). Herbal antimicrobials match rifaximin for SIBO remission. Lactase enzyme reliably eliminates lactose intolerance symptoms. But Klotho supplements, most “fat burner” blends, and heavily marketed whole-food concentrates lack the RCT evidence to justify their price tags.
The Evidence Tier Framework — Tier 1 (strong, replicated clinical evidence), Tier 2 (promising but mixed), Tier 3 (largely marketing) — gives you a permanent decision tool that doesn’t require a medical degree. Apply it to every supplement you encounter: what is the specific clinical trial evidence? What dose was studied? Does the product you’re looking at match the trial parameters? These three questions cut through 90% of supplement marketing immediately. And remember: the framework cuts both ways — even Tier 1 herbs carry real safety risks, especially if you take prescription medications.
Before you start any herbal supplement, run it through the safety checklist in this guide, check the FDA Tainted Products Database, and tell your pharmacist what you’re taking. Start with the herbs that have Tier 1 evidence for your specific condition — Ashwagandha for cortisol, oil of oregano for confirmed SIBO, lactase for dairy intolerance — and give each a proper 8–12 week trial at the clinically studied dose. That’s how you spend your supplement budget on what actually works.
