
⚕️ Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. It is not a substitute for professional medical diagnosis, treatment, or guidance from a licensed physician or physical therapist. Stop any exercise that causes sharp, shooting, or worsening pain and consult a qualified healthcare provider before beginning any new exercise program.
Medically Reviewed by a Licensed Physical Therapist, DPT
If you have hip impingement, you’ve probably been told to “take it easy” — but the real problem isn’t cardio itself. It’s the wrong cardio, done the wrong way. The right cardio exercises for hip impingement, set up correctly, are not just safe — they’re one of the most effective things you can do for long-term joint health.
Here’s what’s at stake if you keep choosing between pain and inactivity: muscle loss, cardiovascular decline, weight gain, and worsening joint stiffness. Every week of unnecessary rest weakens the gluteal and hip stabilizer muscles that protect the joint. That pinching sensation during deep flexion, the flare-up after a run, the frustration of abandoning a workout halfway through — none of that means you’re done with cardio. It means you’ve been using the wrong machines.
In this guide, you’ll learn exactly which cardio exercises are safe for hip impingement, how to set up each machine to stay within a pain-free range, and which movements to eliminate from your routine. Exercise isn’t just possible with FAI — clinical guidelines list it as the first-line treatment.
Low-impact cardio exercises for hip impingement — including the stationary bike, elliptical, and swimming — are safe when movements stay within the FAI Cardio Window (0–90° hip flexion). Research shows that consistent, guided conservative management reduces FAI symptoms in 70–82% of patients (PMC, 2023).
- Stationary bike: Raise the seat higher than normal to avoid deep hip flexion
- Elliptical: Use a moderate stride length; avoid maximum incline
- Swimming: Freestyle and backstroke are safe; avoid whip kicks (breaststroke)
- Avoid: Deep squats, high knees, running on hard surfaces, and rowing ergometers
- The FAI Cardio Window: If the machine keeps your hip below 90° flexion, it’s safe
Understanding Hip Impingement (FAI): What You Need to Know First

Femoroacetabular impingement (FAI) is a condition where abnormally shaped hip bones make contact during movement, causing pain, stiffness, and a characteristic deep pinching sensation in the groin. That contact happens because the femoral head (ball) or acetabular rim (socket) — or both — carry extra bone that crowds the joint space at end-range hip positions. Understanding this mechanism is exactly what makes choosing the right cardio machine so important.
This guide was developed in consultation with physical therapy clinical guidelines, including Fowler Kennedy Sport Medicine’s FAI conservative management protocol and Physiopedia’s peer-reviewed FAI resource. Throughout, we’ll use a simple framework called The FAI Cardio Window to help you quickly identify which machines are safe. More on that shortly.
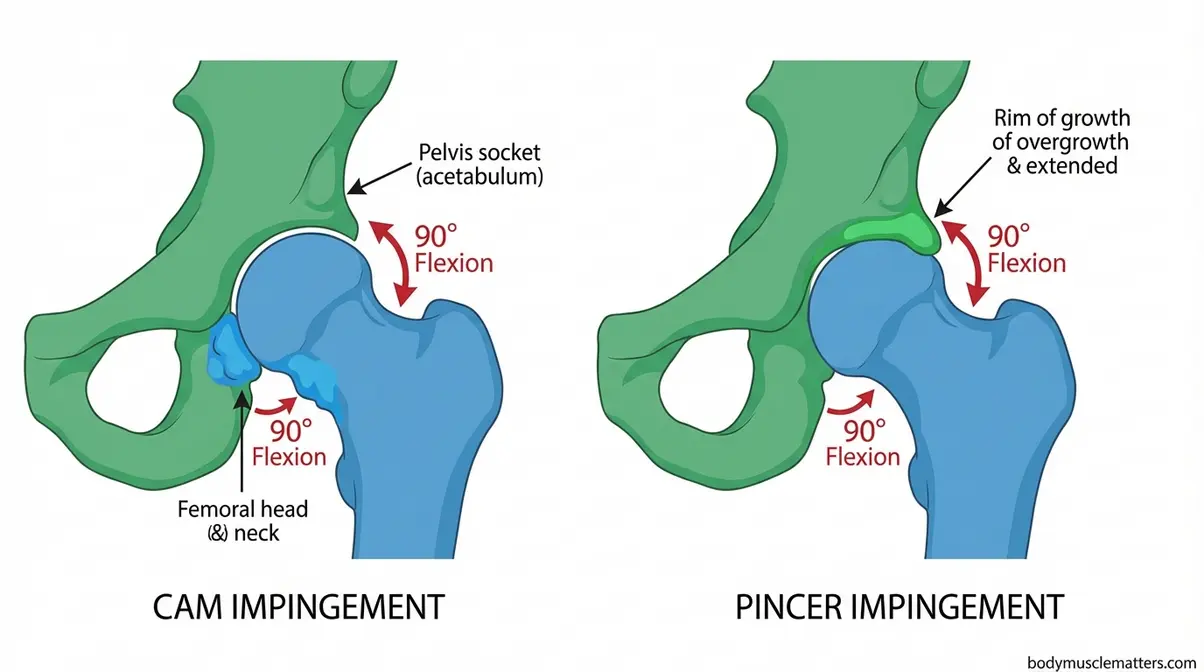
Caption: Cam FAI involves extra bone on the femoral head; pincer FAI involves overgrowth on the socket rim — both cause bone contact during deep hip flexion.
What Is FAI and Why Does It Cause Pain During Cardio?
Hip impingement occurs when abnormal bone shape on the femoral head (cam type) or the acetabular rim (pincer type) causes bone-on-bone contact during specific hip movements. The specific trigger is deep hip flexion — when your knee rises above hip level — combined with internal rotation. Think of it like a door hinge that works smoothly within its normal range but grinds when forced past a certain angle. Within range: fine. At the extremes: painful.
There are two subtypes. Cam FAI features a bump on the femoral head that’s slightly too large for its socket — it grinds when forced to the edge. Pincer FAI involves extra bone on the socket rim that pinches the soft tissue between the rim and femoral neck. Many people have both (mixed type). The key practical point: both types produce pain at the same trigger — deep hip flexion with rotation, exactly what happens during deep squats, high knees, and certain cardio movements.
The reassuring truth is that this is a mechanical, positional problem. The joint is not being permanently damaged by all exercise — only by exercise that forces it into the painful range. Physiopedia’s FAI overview confirms that supervised physiotherapy programs focusing on active core and hip strengthening are significantly more effective for FAI than passive or unsupervised approaches (Physiopedia, 2023).
How Serious Is Hip Impingement?

FAI ranges from mildly symptomatic to severely limiting, but most people do not need surgery. Conservative management — specifically targeted low-impact exercise combined with activity modification — controls symptoms effectively. Research published in PMC (2023) found that non-operative management produces positive outcomes in 70–82% of patients, with improvements in pain and function persisting up to 4–5 years after a structured 12-week physical therapy program.
Left unmanaged, FAI can progress to labral tears and early-onset hip osteoarthritis — which is precisely why doing the right exercise matters more than avoiding exercise altogether. The good news: the right cardio doesn’t just maintain your fitness — research suggests it can actively reduce FAI symptoms over time (PMC, 2023).
With that context in mind, let’s get into the specific cardio exercises that work — and exactly how to set them up.
The Best Cardio Exercises for Hip Impingement

The stationary bike, elliptical machine, swimming, walking, and recumbent bike are the safest cardio exercises for hip impingement. According to peer-reviewed clinical guidelines, bicycling, elliptical training, and stair stepping at moderate intensity are safe cardio modalities for FAI management when performed within a pain-free range of motion (NIH clinical guidelines for FAI exercise, NIH/PMC, 2021). Every recommendation below follows The FAI Cardio Window — the safe range of hip movement, roughly 0–90° of hip flexion, within which your joint can perform cardiovascular exercise without triggering bone-on-bone contact.
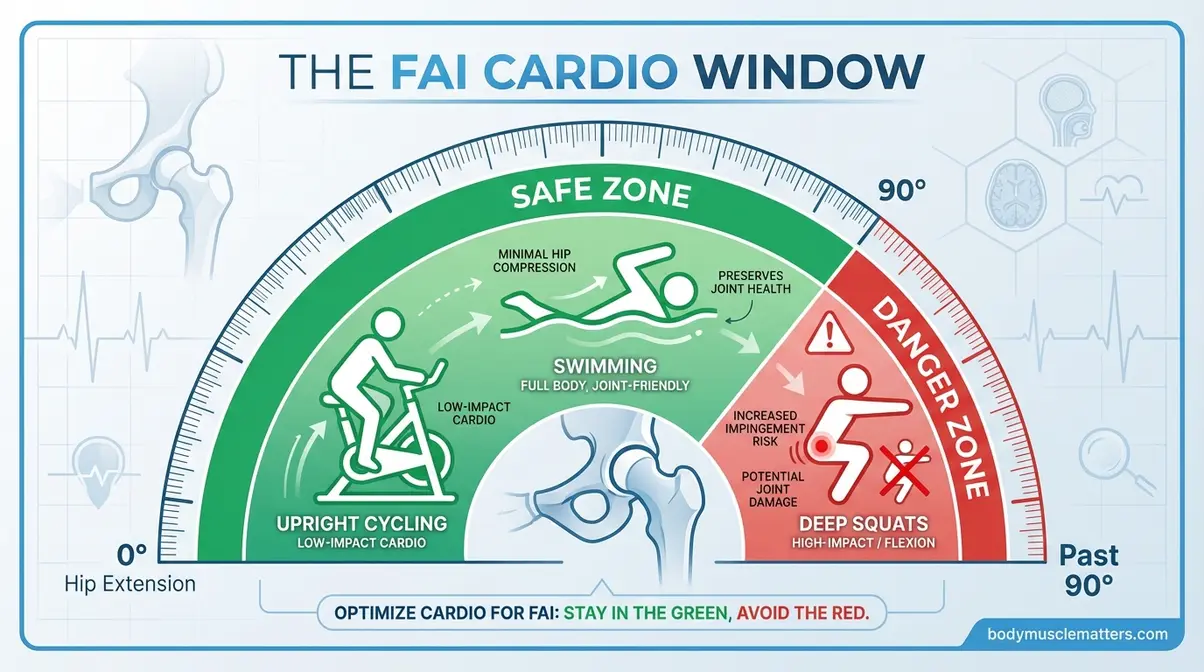
Caption: The FAI Cardio Window marks the 0–90° hip flexion zone where cardio is safe — every machine below keeps you inside it.
These protocols are also relevant for individuals in hip replacement pre-hab, where safe low-impact cardio options for hip impingement overlap significantly with pre-surgical conditioning needs.
Stationary Bike: The Gold Standard Setup for FAI
The stationary bike is the most consistently recommended cardio tool for FAI — and for good reason. The circular pedaling motion is smooth and predictable, with zero impact forces. More importantly, a correctly elevated seat keeps your hip flexion below 90° throughout the entire pedal stroke. As one member of the r/HipImpingement community put it:
“For me it’s walk and bike. You might be able to bike if fitted and with better seat.”
— Community member, r/HipImpingement
That seat adjustment is everything. NIH clinical guidelines for FAI exercise list bicycling among the safe cardio modalities for FAI management (NIH/PMC, 2021). A high seat position means your knee never rises above your hip — you stay within the FAI Cardio Window throughout the pedal stroke.
Exact setup protocol:
- Raise the seat so your knee has a slight bend (10–15°) at the bottom of the pedal stroke — not fully extended, not deeply bent
- Position the seat so that at the top of the stroke, your hip angle stays above 90° — your knee should not exceed hip level
- Sit upright — avoid leaning forward aggressively, which compresses the anterior hip
- Start at low resistance; increase only when you’ve completed 3 consecutive pain-free sessions
- Target 15–20 minutes at moderate intensity (60–70% of maximum heart rate) as your starting point
What to monitor: Stop for sharp, deep pinching in the groin or front of the hip — this is distinct from normal muscle fatigue, which is a burning sensation in the working muscles. If pinching occurs, raise the seat further or reduce resistance before stopping entirely.
The recumbent bike offers an even safer alternative for acute flare-up periods. Its reclined position reduces hip flexion further than the upright version, with slightly lower cardiovascular demand — a worthwhile trade-off when symptoms are elevated.
Where the stationary bike excels in simplicity, the elliptical machine offers a full-body, weight-bearing workout that mimics natural gait — without any of the impact.
Elliptical Machine: Fluid Motion Without the Pinch
“The elliptical’s fluid motion reduces stress on the hips and knees,” notes the Arthritis Foundation, which specifically endorses elliptical training for joint conditions because the motion is guided and controlled (Arthritis Foundation, 2026). Unlike running, there is no heel-strike impact — your feet never leave the pedals, eliminating the compressive spike that occurs at initial contact. The oval track keeps the hip in a consistent, moderate flexion range throughout the stride.
Setup parameters:
- Set stride length to medium — maximum stride length increases hip flexion range and should be avoided
- Keep incline at 0–3° — higher incline increases hip flexion demand at the front of the stride
- Maintain upright posture; do not lean into the handlebars
- Pedal forward only — reverse pedaling increases hip flexor engagement
- Start at 10–15 minutes; progress only when pain-free for 3 consecutive sessions
For FAI patients who want a full-body cardiovascular workout that engages the arms without adding lower-body stress, the elliptical is the strongest option. It provides cardiovascular stimulus comparable to running while keeping joint loading significantly lower — a well-documented advantage for people managing hip and knee conditions (Arthritis Foundation, 2026).
For those whose FAI symptoms are more acute, or who want the lowest possible joint load, swimming removes impact forces entirely.
Swimming and Water Aerobics: Zero-Impact Cardio
Water buoyancy reduces effective body weight by approximately 90% when submerged to the neck — a figure supported by basic hydrostatic physics and applied extensively in physical therapy rehabilitation programs. That near-total offloading of compressive forces makes swimming one of the most joint-friendly cardiovascular options available to anyone managing FAI.
- Safe strokes:
- Freestyle (front crawl): Safe — the hip stays in moderate flexion throughout the kick cycle, never approaching deep flexion
- Backstroke: Safe — the supine position reduces anterior hip compression and keeps the hip in a relaxed, neutral range
- Sidestroke: Generally safe — minimal hip flexion required throughout the stroke
- Strokes to avoid:
- Breaststroke (whip kick): Avoid — the frog-kick motion involves wide hip abduction and external rotation that can directly aggravate FAI. This specific warning is absent from most competitor guides, yet it’s one of the most common pool-based flare-up triggers reported in the FAI community.
Water aerobics classes — aqua jogging, pool walking, and shallow-water resistance work — are an excellent entry point for FAI patients returning to cardio after a flare-up. The controlled environment, combined with the buoyancy offloading, makes it possible to maintain cardiovascular fitness even during symptomatic periods.
Not everyone has pool access. The simplest — and often most underrated — cardio option for FAI is already available to you: walking.
Walking: Short, Frequent Walks Beat Long Distances
Walking can genuinely help manage hip impingement — but session structure matters more than total daily steps. Short, frequent walks (5–15 minutes, 2–3 times daily) are better tolerated than a single 45-minute session, which accumulates fatigue-related gait changes that progressively increase hip loading as muscles tire.
Surface and incline matter too. Flat, firm surfaces — a treadmill or paved path — are preferred over uneven terrain, which demands constant micro-adjustments that increase hip rotation. A slight treadmill incline (1–2%) can actually reduce anterior hip compression compared to flat walking by shifting weight distribution slightly rearward. Avoid steep hills and soft sand, both of which require deeper hip engagement.
A practical starting protocol: three 10-minute walks per day on flat surfaces, progressing by 2 minutes per session only when you’ve been pain-free for the previous two sessions. Brisk walking — not leisurely — provides meaningful cardiovascular benefit while maintaining a controlled, consistent gait pattern.
Beyond these four core options, a handful of additional low-impact activities offer variety without adding joint stress.
Additional Safe Options: Recumbent Bike and Hiking
- Recumbent bike: Even safer than the upright stationary bike because the reclined position reduces hip flexion further. Ideal for acute flare-up periods. Slightly lower cardiovascular demand than upright cycling, but an excellent option when symptoms are elevated. These protocols are also appropriate for hip replacement pre-hab, where low-impact options overlap with FAI-friendly cardio.
- Hiking (moderate terrain): Safe on moderate, even surfaces. The key caveat: avoid steep descents, which force deep knee and hip flexion simultaneously. Use trekking poles on downhill sections to offload the hip and maintain upright posture.
- Aqua jogging (water running): Provides running-equivalent cardiovascular stimulus with near-zero joint impact. Requires a flotation belt. Excellent for maintaining aerobic fitness during acute flare-up periods when even walking is uncomfortable.
One important note: stair climbers and rowing ergometers are sometimes marketed as “low-impact,” but both force the hip past 90° of flexion — they fall outside the FAI Cardio Window and are covered in the next section.
Knowing what’s safe is only half the equation — knowing what to avoid is equally important.
Exercises and Activities to Avoid with Hip Impingement

Two categories of exercise reliably trigger FAI symptoms: high-impact activities that generate excessive joint compression, and deep hip flexion movements that push the hip past the safe threshold. All of the exercises below share one thing: they force the hip past the FAI Cardio Window — the 90° boundary where bone-on-bone contact occurs. Avoiding these movements does not mean abandoning fitness; it means redirecting effort toward the machines and protocols in the previous section.
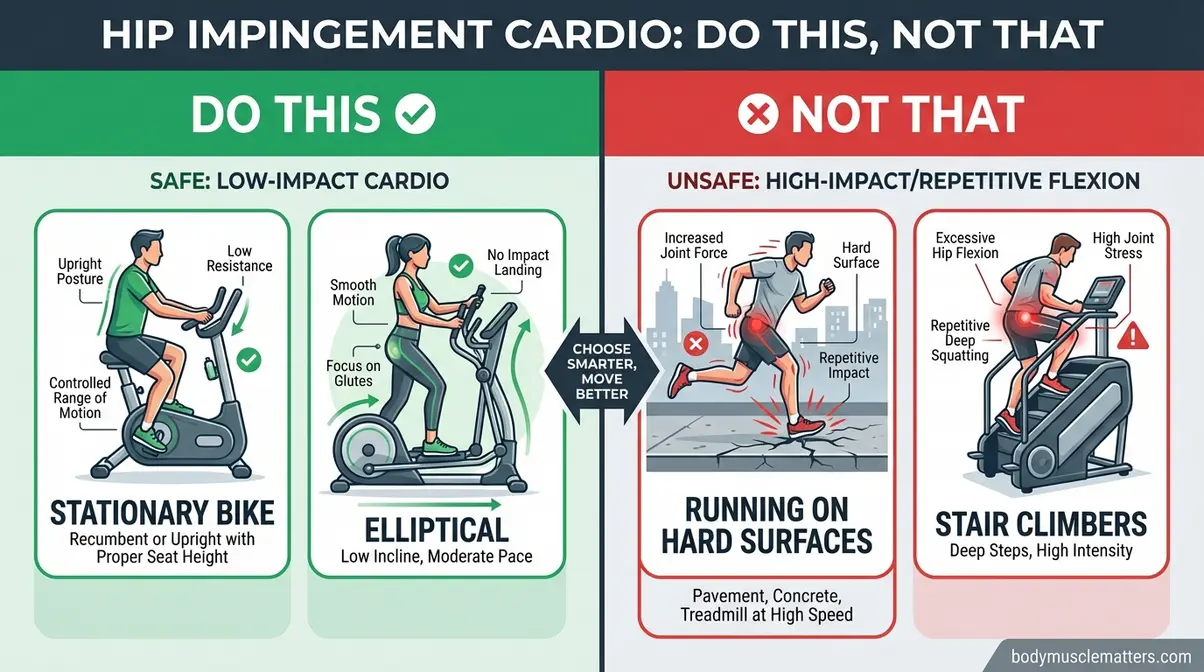
Caption: Side-by-side comparison of FAI-safe cardio choices (stationary bike, elliptical, swimming) versus movements that trigger bone-on-bone contact.
High-Impact Activities That Worsen Joint Compression
Running on hard surfaces is the most common cardio trigger for FAI flare-ups. Repetitive heel strike generates 2–3× body weight in joint loading with each step. For FAI, this compressive force — combined with the hip flexion required at initial contact — accelerates pain. Treadmill running on a cushioned surface is marginally better but remains problematic during symptomatic periods. If running is important to you, treat it as a goal to return to after symptoms stabilize, not a current option.
Jumping exercises — jumping jacks, box jumps, and burpees — generate landing forces of 4–8× body weight. The sudden, uncontrolled hip flexion at landing is particularly problematic for FAI because the joint has no time to decelerate gradually. These should be eliminated entirely during symptomatic phases.
Stair climbers deserve a specific warning. Despite being marketed as low-impact, the stair climber requires the hip to flex repeatedly past 90° with each step cycle. This directly violates the FAI Cardio Window. Many users with FAI report stair climbers as one of their most consistent flare-up triggers — a pattern worth noting even if the machine feels manageable on good days.
- Exercises to avoid in this category:
- Running on concrete, asphalt, or hard gym floors
- Jumping jacks, box jumps, burpees, jump rope
- Stair climbers and step aerobics classes
- Any sport involving repeated jumping or hard landings (basketball, volleyball)
For patients who need to avoid all lower-body cardio during a flare-up, cardio exercises without using your legs provide a viable alternative for maintaining cardiovascular fitness.
Impact forces are one half of the problem. The other half is deep flexion — movements that bend the hip past its safe range regardless of whether they’re high or low impact.
Deep Flexion Movements to Eliminate From Your Routine
Deep squats are among the most aggravating exercises for FAI. When the hip descends below parallel, it crosses the FAI Cardio Window threshold. The compressive force at the bottom position is amplified by the narrowed joint space characteristic of FAI morphology. Some patients tolerate bodyweight squats to 60–70° of flexion (above parallel), but this should be cleared with a physical therapist before attempting.
Heavy lunges present a dual problem: the forward knee drive forces deep hip flexion on the lead leg while simultaneously loading the hip flexor on the trailing leg. Reverse lunges are marginally safer but still risky during active flare-up periods.
High knees and rowing ergometers both explicitly drive the hip past 90°. High knees do so with every repetition — it’s built into the movement pattern. The rowing ergometer is a less obvious but equally problematic entry: at the “catch” position (knees fully bent, body compressed forward), the hip reaches near-maximum flexion under load. This specific trigger is absent from virtually every competitor guide, yet it catches many FAI patients off guard who assume rowing is joint-friendly.
Cycling with a low seat is a counterintuitive hazard. A seat set too low forces deep hip flexion at the top of the pedal stroke — turning one of the safest exercises in this guide into a harmful one. This is why exact setup parameters matter as much as machine selection.
The Cleveland Clinic’s low-impact cardio guidance recommends avoiding high-impact and deep flexion exercises for hip joint conditions, endorsing swimming, cycling, and elliptical training as safer alternatives (Cleveland Clinic, 2024).
Knowing which exercises to avoid in the gym is essential. But FAI flare-ups don’t only happen during workouts — several everyday activities can trigger pain just as reliably.
What Flares Up Hip Impingement? Daily Triggers Explained

FAI flare-ups are triggered by any activity — inside or outside the gym — that pushes your hip past the FAI Cardio Window. The most common triggers fall into two groups: exercise-related overload and daily life positions that accumulate hip flexion over hours rather than minutes. Prolonged sitting in low chairs, car seats, and deep sofas forces the hip into sustained flexion past 90° — one of the most common non-exercise triggers for FAI flare-ups. Understanding both categories helps you manage total hip load across the day, not just during workouts.
Exercise-Related Flare-Up Triggers
Three exercise patterns consistently produce flare-ups even when the machine choice is correct.
Rapid progression is the most common culprit. Jumping from 10 minutes of elliptical to 40 minutes in a single week gives FAI tissues no time to adapt. The 10% weekly progression rule — increase session duration by no more than 10% per week — exists precisely to prevent this. If you’re doing 20 minutes pain-free, move to 22 minutes the following week, not 30.
Fatigue-related form breakdown is subtler but equally damaging. As the gluteal muscles and hip abductors fatigue, compensatory movement patterns emerge — the pelvis drops, the knee tracks inward, and hip flexion increases. A 20-minute session with consistent form is safer than a 40-minute session where mechanics deteriorate in the final quarter. This is one reason why multiple shorter sessions outperform one long session for FAI management.
Starting cold is an underappreciated trigger. Without a 5-minute warm-up of gentle movement — hip circles in a pain-free range, slow walking, standing hip pendulum swings — the synovial fluid in the hip joint hasn’t distributed fully. Early-session pinching is significantly more common when the warm-up is skipped.
For patients who experience lower back tightness alongside FAI symptoms, techniques for relieving tight lower back muscles can address the compensatory patterns that develop when hip mobility is restricted.
Exercise triggers are the ones most people are aware of. But daily life — not the gym — is where many FAI patients accumulate the most aggravating hip flexion.
Daily Life Triggers: Stairs, Sitting, and Posture
The following daily positions are among the most common non-exercise FAI triggers — and the least discussed:
- Stairs: Stair climbing requires 90–120° of hip flexion per step, which routinely pushes the hip past the FAI Cardio Window. Going up stairs is generally more aggravating than going down. Modification: take stairs one at a time, leading with the non-affected leg, and use the handrail to partially offload the hip.
- Prolonged sitting in low chairs: A deep sofa, low car seat, or bucket seat holds the hip in sustained flexion past 90°. The sustained compression — not just the angle — is what aggravates FAI over time. Modification: use a firm seat cushion to raise seated height; stand and take a brief walk every 30 minutes during prolonged sitting.
- Sleeping position: The fetal position holds the hip in deep flexion for hours at a time, often contributing to morning stiffness and early-day flare-ups. Recommendation: sleep on your back with a pillow under your knees, or on the unaffected side with a pillow placed between your knees to prevent the top hip from dropping into internal rotation.
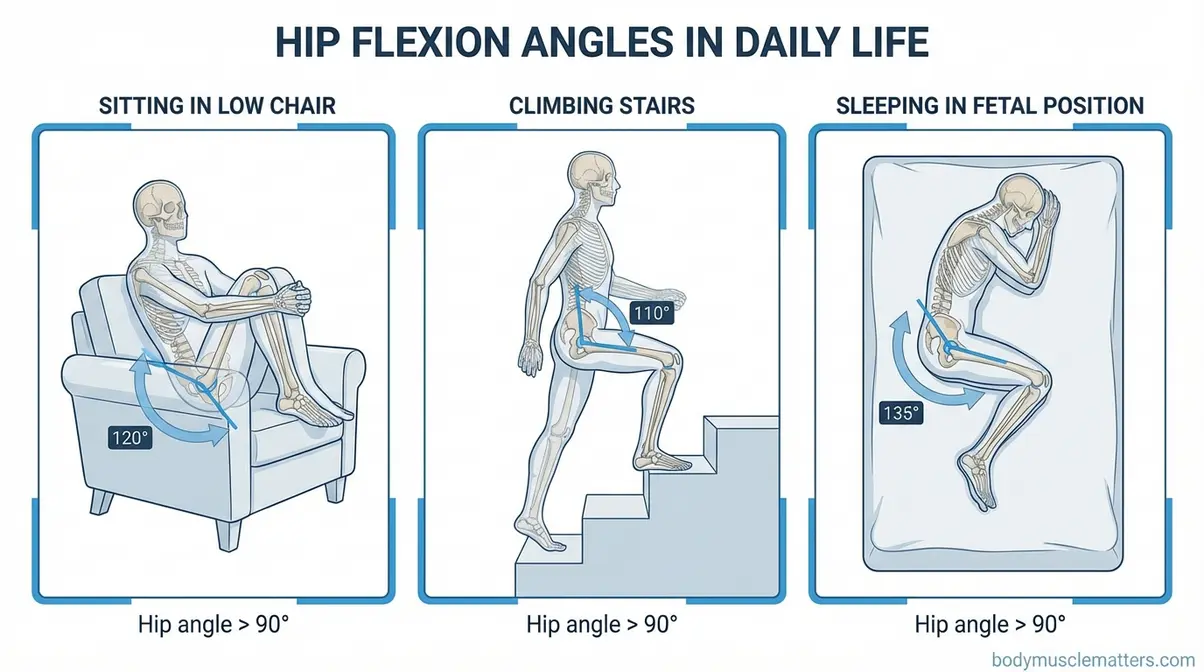
Caption: Common daily positions that push the hip past 90° — the same threshold that triggers FAI pain during exercise.
Now that you know what triggers flare-ups, here’s how to structure your cardio sessions to stay consistently within a safe range — without giving up fitness.
Tips for Safe Cardio with Hip Impingement
Safe cardio for FAI is about controlling three variables: hip flexion angle, session duration, and progression rate. The FAI Cardio Window provides the guiding principle for angle — every tip below addresses the other two variables. Maintaining cardio intensity at 60–70% of maximum heart rate keeps cardiovascular load therapeutic while minimizing the compressive hip stress that accumulates at higher exertion levels.
Follow these six strategies to build a consistent, pain-free cardio routine:
- Warm up for 5 minutes before every session. Gentle hip circles, standing hip pendulum swings within a pain-free range, and slow walking prime the synovial fluid and reduce early-session stiffness. This single habit reduces first-10-minutes flare-ups more than any equipment adjustment.
- Target 60–70% of maximum heart rate. This intensity provides cardiovascular benefit without the muscle fatigue that leads to compensatory movement patterns. Use the formula 220 − age to estimate your maximum heart rate, then multiply by 0.6–0.7. A 40-year-old targets 108–126 beats per minute.
- Apply the 10% progression rule. Increase session duration by no more than 10% per week. If you’re completing 20 minutes pain-free, progress to 22 minutes the following week — not 30. FAI symptoms often manifest 24–48 hours after activity, a delayed response that catches many patients off guard.
- Use a pain monitoring scale throughout the session. Rate your pain 0–10. At 0–3: continue as planned. At 4–5: modify immediately — reduce resistance, shorten stride length, or raise the bike seat. Above 5: stop and rest. This is the practical, real-time application of the FAI Cardio Window.
- Release hip tension after cardio. Gentle hip flexor stretches — a standing lunge stretch with an upright torso, or a supine knee-to-chest stretch taken only to 90° — reduce post-exercise stiffness. Avoid aggressive hip flexor stretches that force the hip past 90°, which can trigger post-workout flare-ups.
- Build rest days into your schedule. Allow 1–2 rest days between cardio sessions during the initial phase. If you’re new to structured FAI management, three sessions per week is a sensible starting point before progressing to four or five.
For patients who want to complement cardio with gentle strength work, beginner at-home strength and mobility exercises provide a compatible starting framework that supports hip stabilizer development without deep flexion loading.
These strategies work best when FAI is in a manageable phase. If symptoms are severe, persistent, or worsening, the situation calls for professional evaluation — not more self-management.
Limitations and When to Seek Professional Help
Self-managed exercise is a powerful tool for FAI — but it has real limits. This section is not meant to alarm you; it’s meant to give you clear, specific thresholds so you know when to act. Physical therapists and orthopedic specialists are your partners in this process, not a last resort.
Common Pitfalls When Managing FAI Independently
Pitfall 1 — Exercising through sharp pain: Fitness culture often promotes “pushing through discomfort,” but sharp, deep pinching in the groin during exercise is not normal discomfort — it’s a mechanical signal. Continuing through that sensation risks acute labral irritation and, over time, labral tear progression. Use the 0–10 pain scale from the previous section: stop at 5/10. Stop any exercise that causes sharp, shooting, or worsening pain and consult a physical therapist or physician immediately.
Pitfall 2 — Stopping all activity during a flare-up: A painful day does not warrant two weeks of complete rest. Total inactivity weakens the gluteal support structures that protect the joint, making the next session more likely to cause pain — a cycle that’s hard to break. Instead, substitute low-load alternatives: pool walking, gentle walking on flat ground, or upper-body cardio until symptoms settle.
Pitfall 3 — Self-diagnosing without imaging confirmation: Hip pain during deep flexion is a symptom shared by several conditions, including hip bursitis, labral tears without FAI morphology, and hip flexor tendinopathy. Following an FAI protocol for the wrong condition can delay appropriate care. Confirm diagnosis with X-ray or MRI before committing to a targeted protocol.
When Conservative Management Isn’t Enough
Conservative management typically produces measurable improvement within 6–12 weeks. Research from PMC (2023) shows that non-operative treatment — targeted exercise, activity modification, and physical therapy — reduces symptoms in the majority of patients, with outcomes lasting up to 5 years. Sanford Health’s non-operative FAI guideline notes that 6–8 weeks of supervised physical therapy is usually sufficient to determine whether conservative care is working.
If your symptoms are not improving after 12 weeks of consistent, guided conservative management, escalation is appropriate. The typical pathway: GP or orthopedic evaluation → imaging confirmation (X-ray/MRI) → corticosteroid injection for acute pain relief → arthroscopic surgery for structural correction if conservative management fails. The Hospital for Special Surgery exercise guidance confirms that progressive exercise under professional guidance is critical for managing hip joint conditions, with professional support essential for complex presentations (HSS, 2024).
For patients progressing toward surgery, pre-operative exercise (“prehab”) is strongly recommended to improve post-surgical outcomes. Upper-body conditioning and low-load core work can maintain fitness while protecting the hip. Complementary work on exercises for scapular health and mobility supports posture and upper-body conditioning during this phase.
Before we wrap up, here are direct answers to the most common questions readers ask about cardio and hip impingement.
Frequently Asked Questions
What cardio machine is best for hip impingement?
The stationary bike and elliptical machine are the best cardio options for hip impingement. Both provide fluid, low-impact motion that keeps the hip within a safe flexion range throughout the movement. The elliptical eliminates heel-strike impact entirely, while the stationary bike offers a fully controlled, seated position with no balance demands. For the stationary bike, raise the seat so your knee angle at the top of the pedal stroke stays above 90° — this single adjustment is the difference between a therapeutic session and a painful one. If either machine causes sharp groin pain or pinching, consult a physical therapist before continuing.
What exercises should I avoid for hip impingement?
Avoid high-impact activities and movements requiring deep hip flexion — specifically any exercise where your knee rises above hip level under load. The primary offenders: deep squats, heavy lunges, high knees, jumping jacks, fast running on hard surfaces, and rowing ergometers. These movements force the hip past 90° of flexion, triggering bone-on-bone contact at the FAI zone. Stair climbers are a less obvious but equally problematic machine — the step motion repeatedly drives the hip past the safe threshold. Movements that keep the hip below 90° of flexion are generally safe; confirm with a PT for your specific presentation.
Will I ever exercise again properly with hip impingement?
Yes — most people can exercise again with hip impingement with the right approach. Research shows that tailored low-impact cardio, core strengthening, and hip stabilization effectively reduce symptoms in 70–82% of patients following structured conservative management (PMC, 2023). Many return to full cardiovascular training within 8–12 weeks of guided exercise. The key is not pushing through pain but building systematically within the FAI Cardio Window. Working with a physical therapist to modify movements and avoid deep hip flexion is the most reliable path back to full activity.
Can walking help hip impingement?
Walking can help manage hip impingement when structured correctly. Short, frequent walks — 5–15 minutes, two to three times daily — are better tolerated than single long sessions, which accumulate fatigue-related gait changes that increase hip loading. Walking on a slight treadmill incline (1–2%) can actually reduce anterior hip pressure compared to flat walking. Start with three 10-minute walks per day on flat surfaces and progress by 2 minutes per session only when pain-free. If walking causes deep groin pain or pinching that persists after the session, reduce distance and consult a physiotherapist.
What flares up hip impingement?
FAI flare-ups are triggered by repetitive or deep hip flexion, internal rotation, and high-impact forces. Specific exercise triggers include deep squatting, running on hard surfaces, high knees, stair climbers, and rowing ergometers. Daily life triggers are equally important: prolonged sitting in low chairs or car seats, stair climbing, and sleeping in the fetal position all hold the hip in sustained or deep flexion. Even sitting in a low car seat or deep sofa for extended periods can trigger a flare-up by compressing the joint over time. Avoiding these triggers and applying the 10% progression rule when returning to exercise helps prevent acute inflammation.
Putting It Together: Your FAI Cardio Plan
For adults managing hip impingement, cardio exercises for hip impingement are not just tolerated — they’re clinically recommended as first-line treatment. Research shows that consistent, guided conservative management reduces FAI symptoms in 70–82% of patients over 8–12 weeks (PMC, 2023). The best approach combines a correctly set-up stationary bike or elliptical, short structured walking sessions, and swimming with safe strokes — all performed within the 0–90° hip flexion range that protects the joint.
The FAI Cardio Window is the mental model that makes all of this actionable. You don’t need to memorize a list of forbidden exercises — you need one question: “Does this movement keep my hip below 90° of flexion?” If yes, it’s likely safe. If no, it’s likely a trigger. That single principle covers the stationary bike seat height, the elliptical stride setting, the swimming stroke selection, and the stair climber avoidance. You came into this article worried that cardio would make your hip worse. Leave with a clearer picture: the right machines, set up correctly, actively support recovery.
Start this week: 15 minutes on a high-seat stationary bike at 60–70% of your maximum heart rate. If you’re pain-free after three sessions, add 5 minutes. Progress from there using the 10% weekly rule. If symptoms persist beyond 6–8 weeks of consistent effort, consult a physical therapist for individualized assessment — that’s not a setback, it’s the smart next step.
⚕️ Medical Disclaimer: The information in this article is for educational purposes only. It does not constitute medical advice and is not a substitute for professional diagnosis, treatment, or guidance from a licensed physician, physical therapist, or other qualified healthcare provider. Always consult a qualified professional before starting a new exercise program, especially if you have a diagnosed condition like femoroacetabular impingement (FAI).
